Targeted Treatment
Yttrium-90
Radioembolization

Indiana University School of Medicine
November 19, 2025
Hepatocellular Carcinoma
Liver cancer ranks as the 6th most common cancer and 3rd leading cause of cancer-related death worldwide
Hepatocellular carcinoma represents 75-85% of all liver cancer cases wordwide.
5-year survival rates in the U.S. have risen from 3% (1975-1977) to 22% (2014-2020)

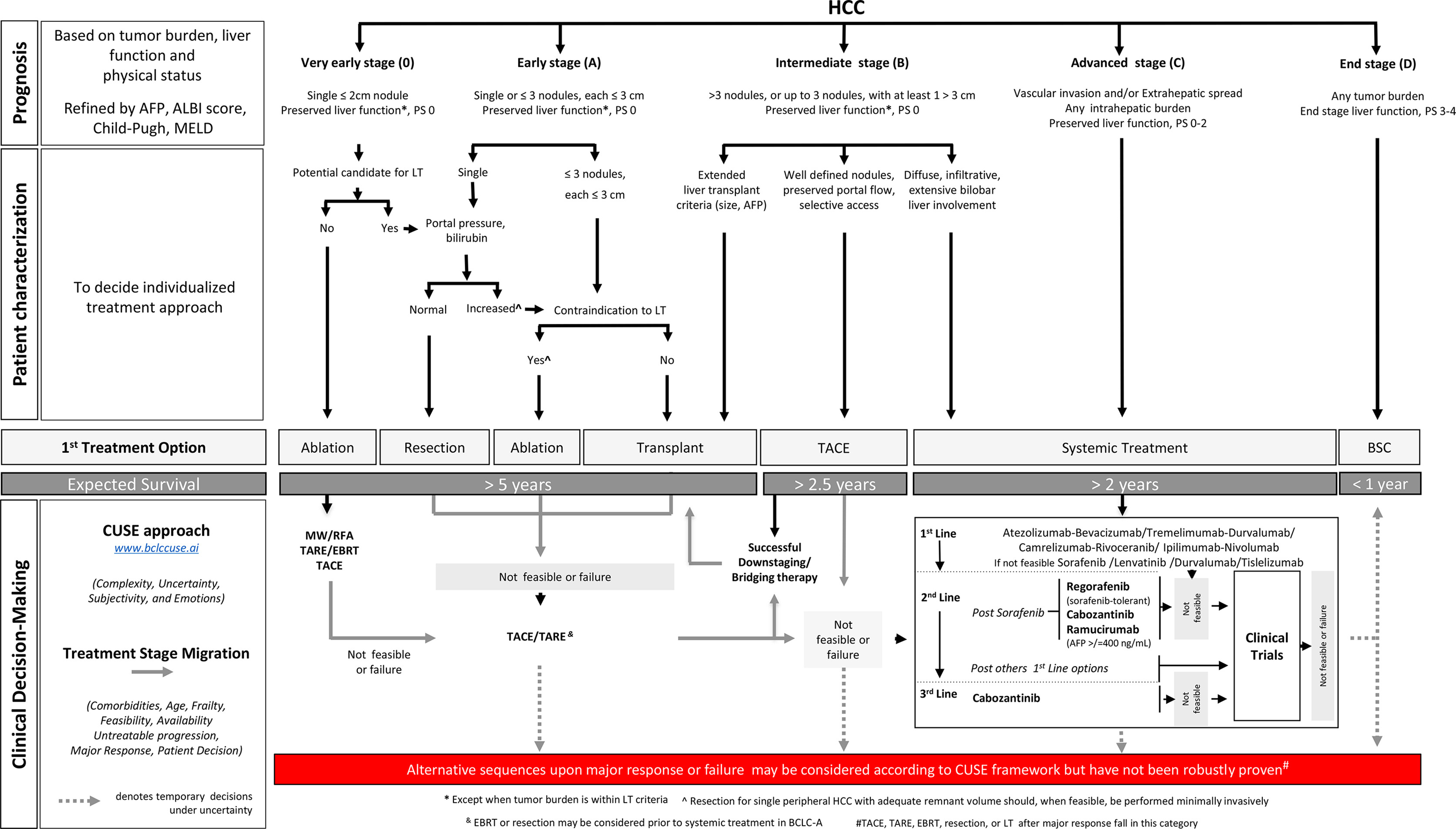
Where Y90 Fits Diagnosis
Y90 is suited for liver-dominant disease, especially:
BCLC A tumors not amenable to ablation
BCLC B intermediate tumors
Select BCLC C patients with portal vein thrombosis
1960s - 1990s
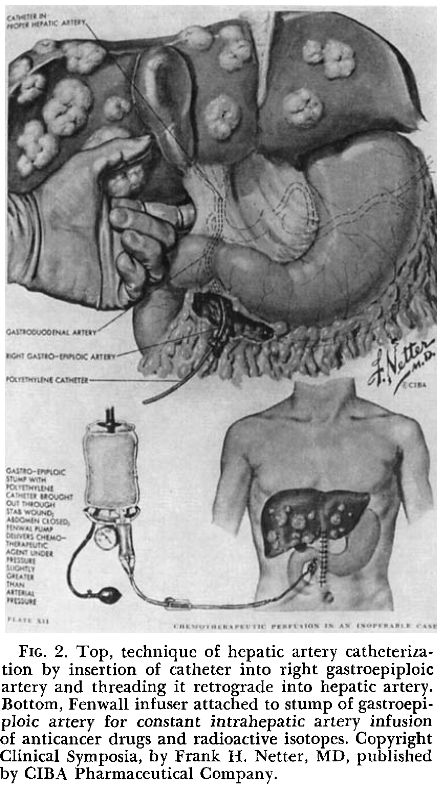
In 1951, Bierman et al demonstrated angiographically that liver tumors received their blood supply from the hepatic artery and not the portal vein.
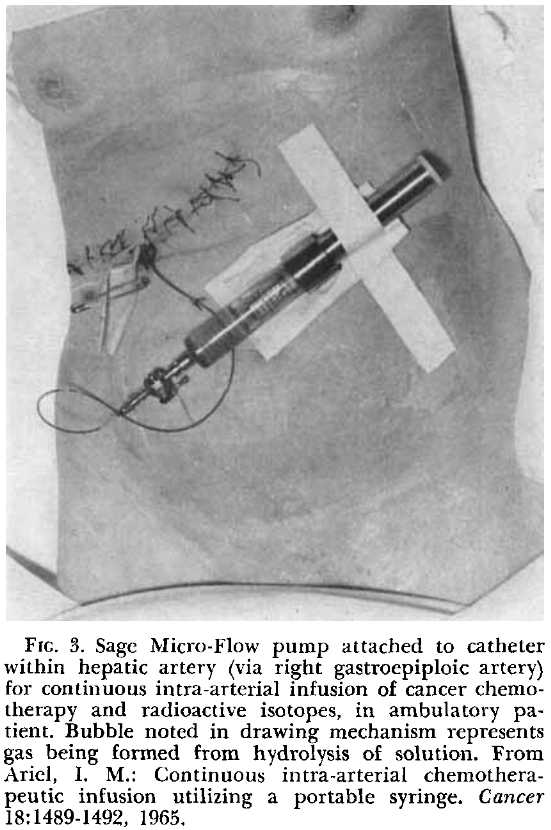
1967, Ariel & Pack perform first Y90 administration in four patients
2000s - Present
1999: TheraSphere granted a humanitarian device exemption for use in patients with unresectable HCC.
2016: SIR-Spheres approved for the treatment of unresectable metastatic liver tumors from primary colorectal cancer with adjuvant intrahepatic artery chemotherapy.
2025: SIR-Spheres for the treatment of unresectable hepatocellular carcinoma (HCC) following the DOORwaY-90 study


SARAH Trial
Phase III, open-label, randomized controlled trial
\(^{90}\)Y Resin Microspheres vs. Sorafenib for advanced HCC (BCLC C)
No significant difference in overall survival (8.0 months for Y90 vs. 9.9 months for sorafenib)
Radioembolization associated with fewer adverse events and better quality of life
SIRveNIB Trial
Phase III, open-label, randomized controlled trial
\(^{90}\)Y Resin Microspheres vs. Sorafenib for advanced HCC (BCLC B or C) in the Asia-Pacific
No significant difference in overall survival (8.8 months for Y90 vs. 10.0 months for sorafenib)
Radioembolization showed significantly fewer grade 3 adverse fewer adverse events (27.7% vs. 50.6%)
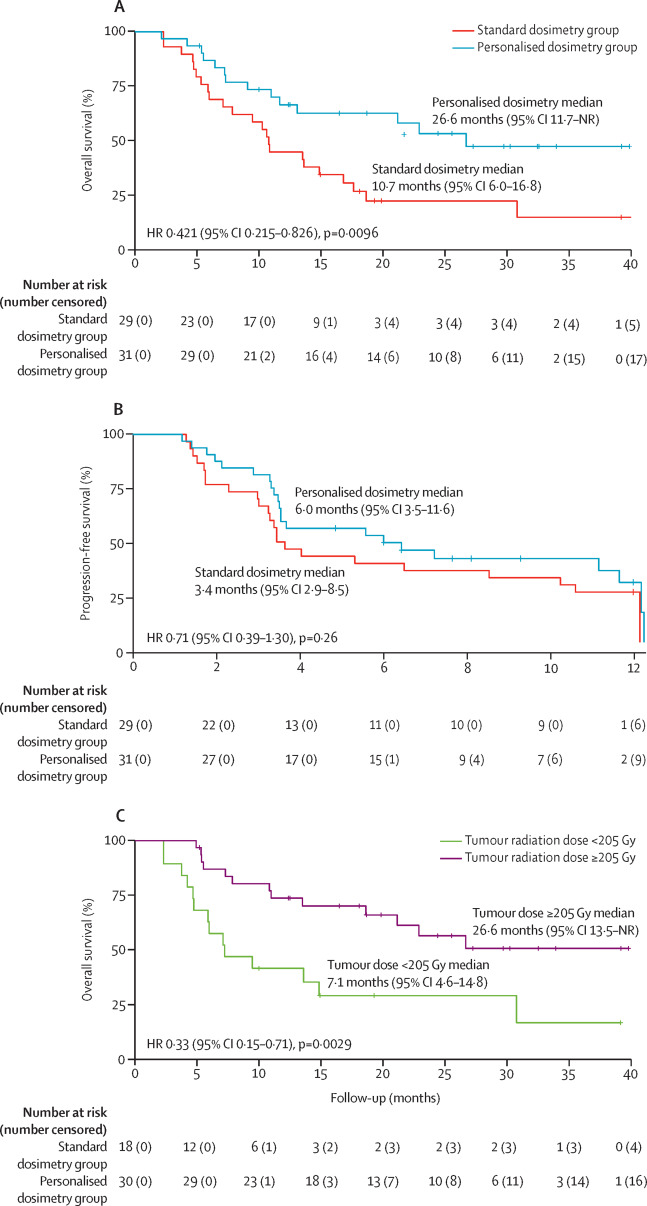
DOSISPHERE-01 Trial
Phase III, open-label, randomized controlled trial
Personalized Dosimetry (≥205 Gy target) vs. Standard Dosimetry (∼120 Gy target)
Personalized dosimetry showed higher median overall survival (26.6 months for vs. 10.7 months)
Also showed higher tumor responses response rates (71% vs. 36%) and increased rates of downstaging to surgical treatments (35% vs. 3.5%)
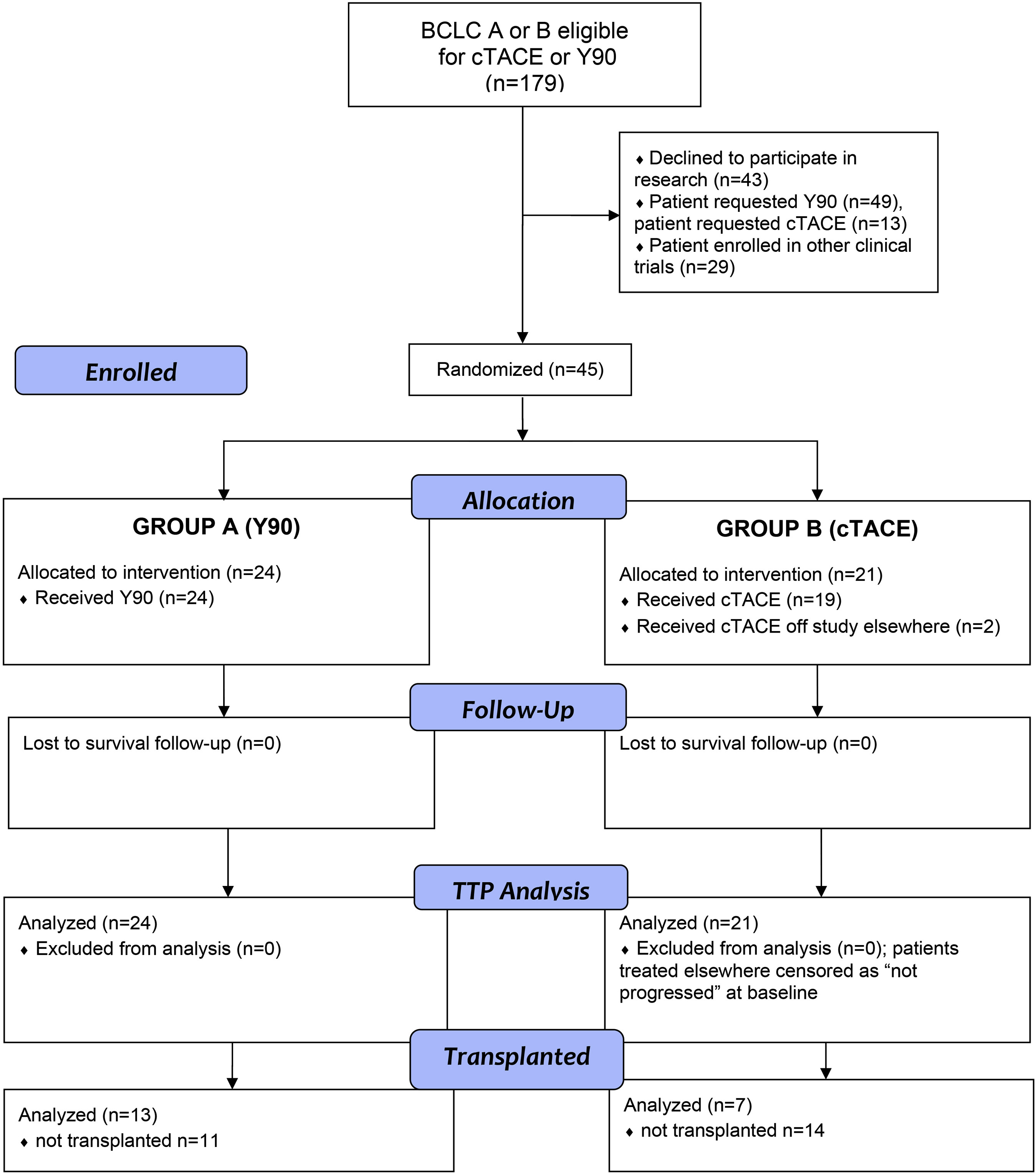
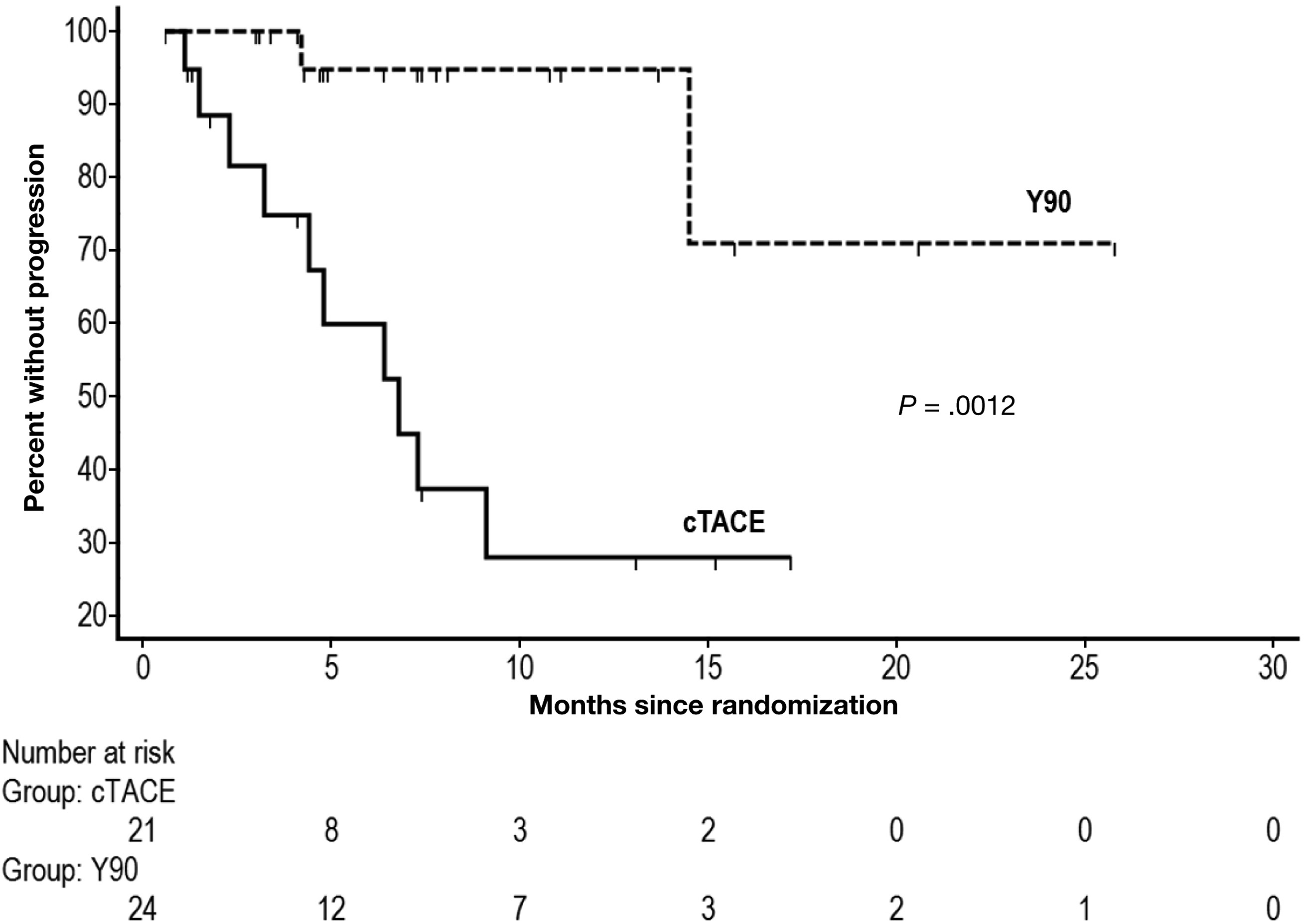
TRACE Trial
Y90 Radioembolization vs. Drug-Eluting Bead Chemoembolization (DEB-TACE)
The trial was stopped early because the primary endpoint (TTP) was met in favor of Y90
Y90 TARE showed superior median overall (30.2 months vs. 15.6 months)
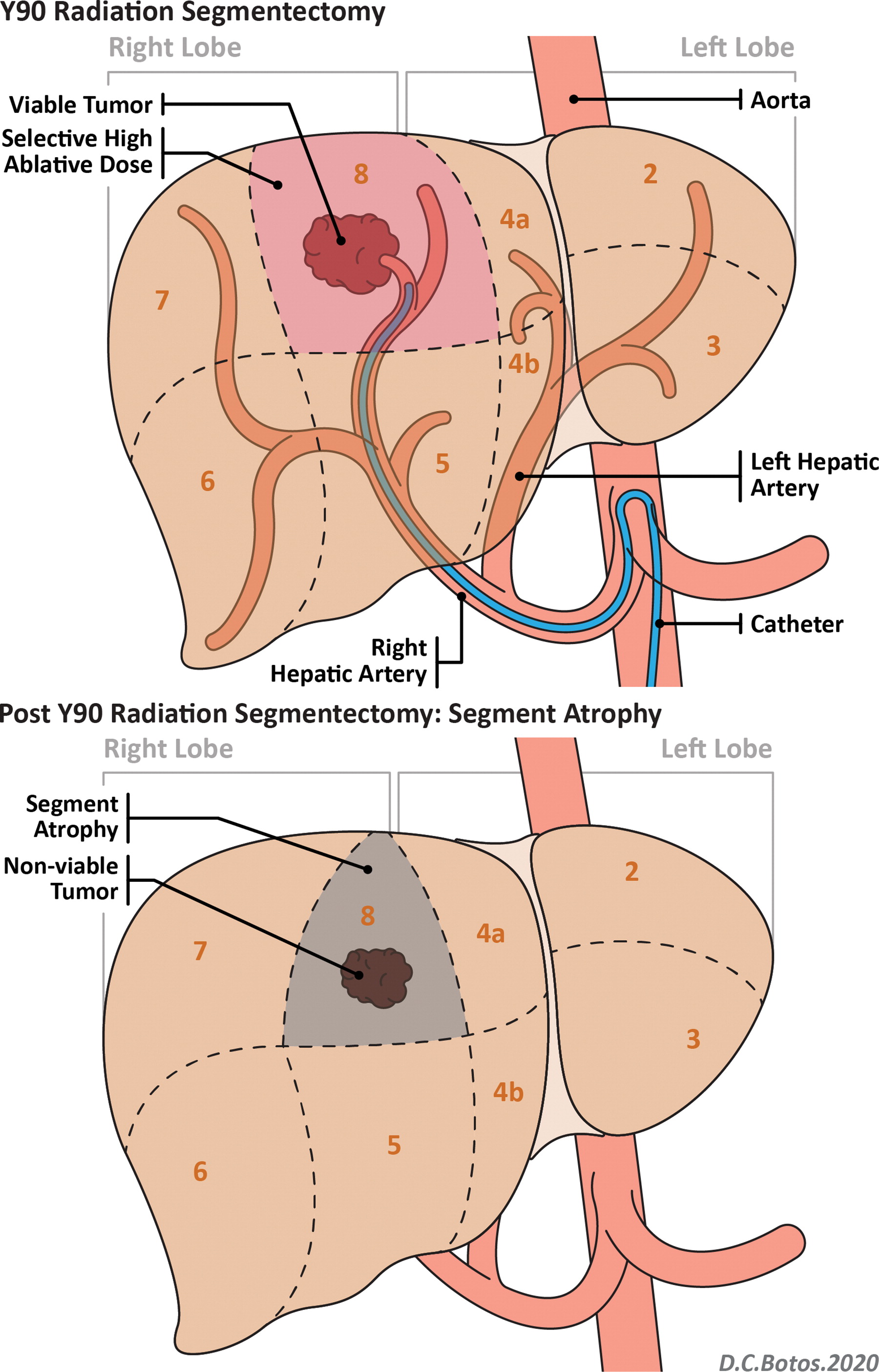
Radiation Segmentectomy
Superselective infusion of a very high dose (> 400 Gy)
Evidence:
- LEGACY trial: ORR 90%, median OS ~45 months
Pearls:
- Identify variant anatomy (parasitizing supply, accessory/replaced vessels)
- Different segments are associated with different post-embolization complications
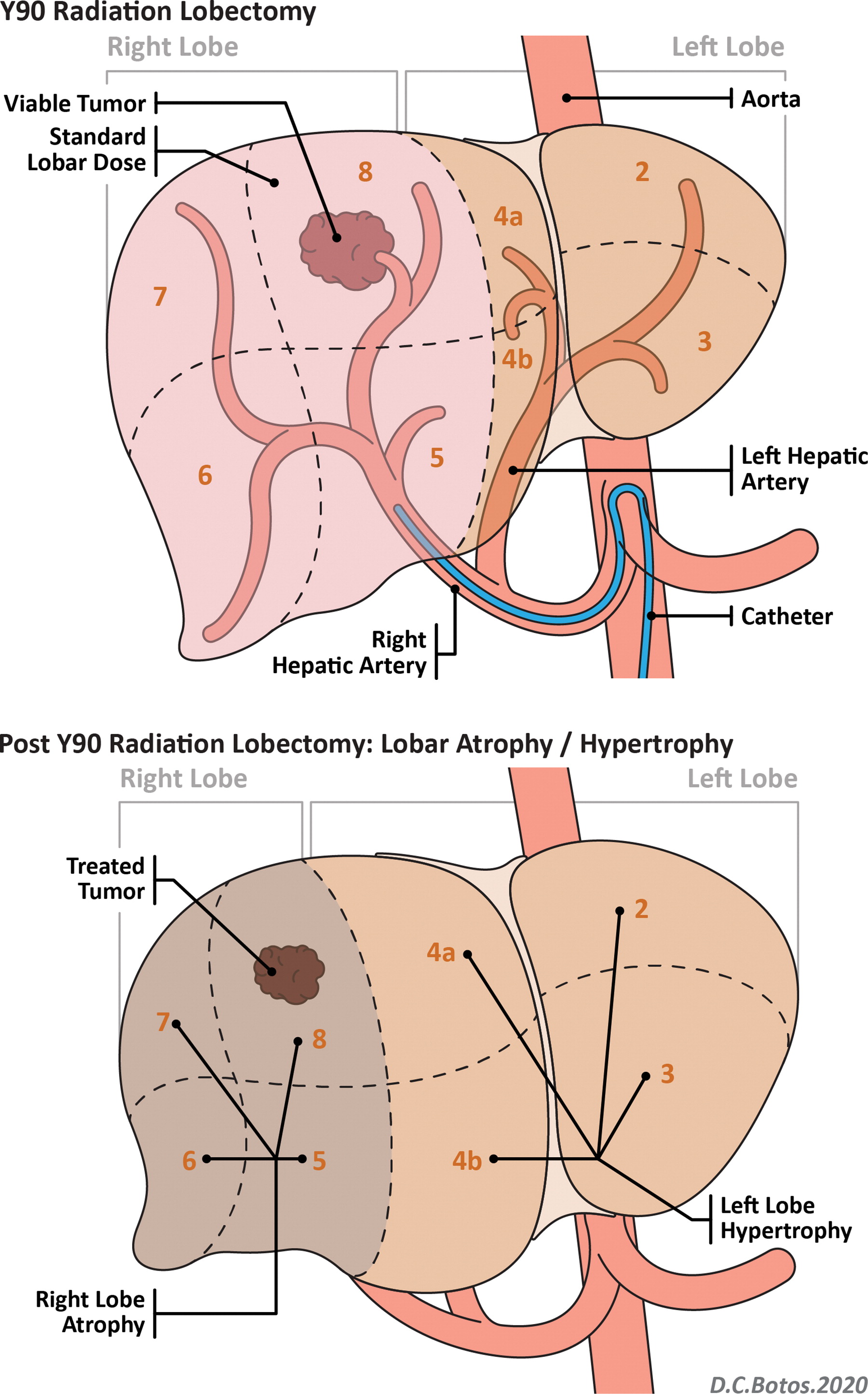
Radiation Lobectomy
Lobar dose to induce hypertrophy of the contralateral lobe
Alternative to portal vein embolization
Provides tumor control while waiting for future liver remnant (FLR) growth
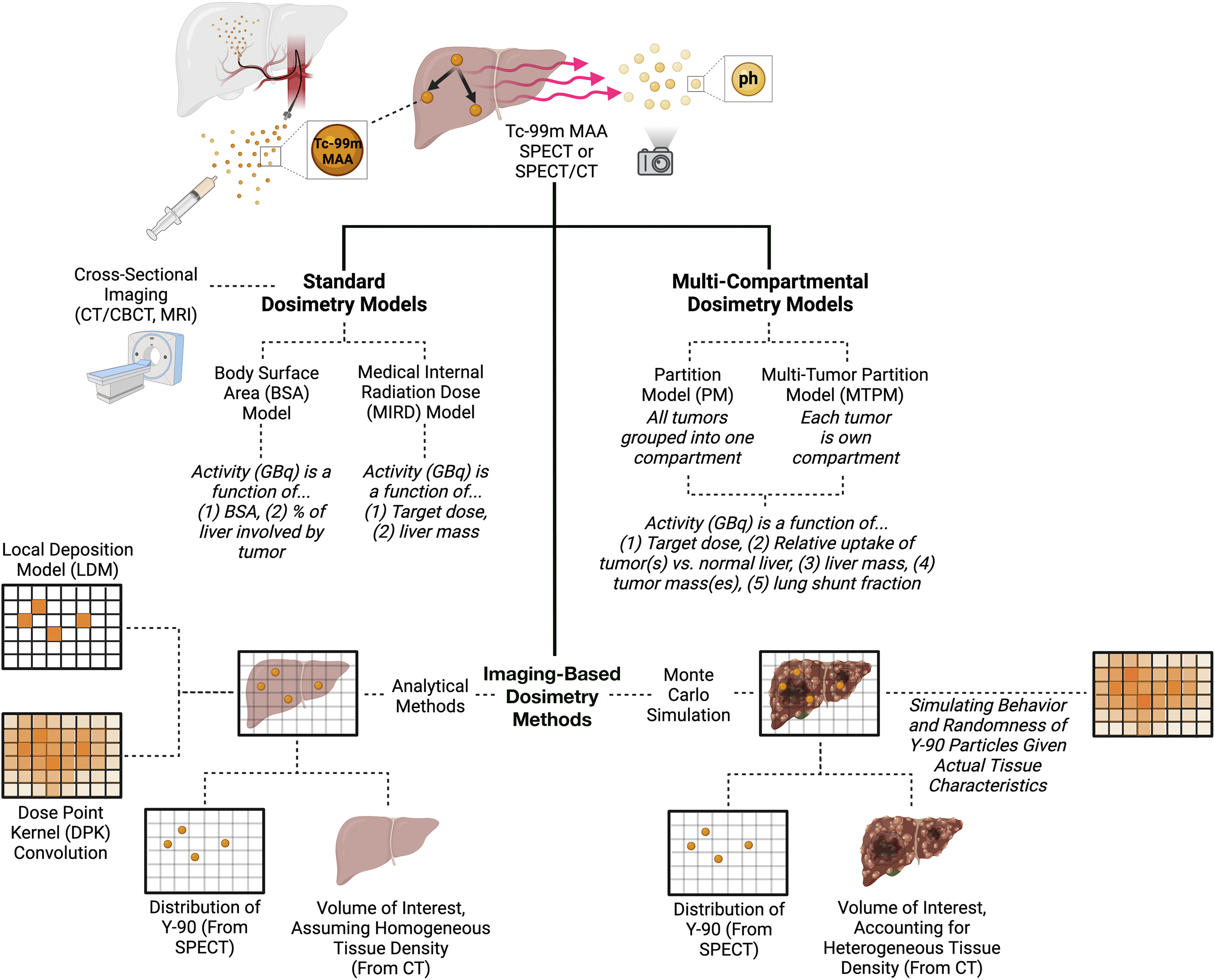
Personalized Dosimetry
Old model: everyone gets the same dose
Modern model
99mTc-MAA SPECT/CT
Voxel- or partition-based dosimetry
Targeted dose delivery
Evidence
- DOSISPHERE-01: OS 10.7 → 26.6 mo
Patient Selection

Patient Selection
Patient Selection
Child-Pugh A and early B
Liver-dominant disease
Assess vascular anatomy and shunting
Multidisciplinary input with hepatology and surgery
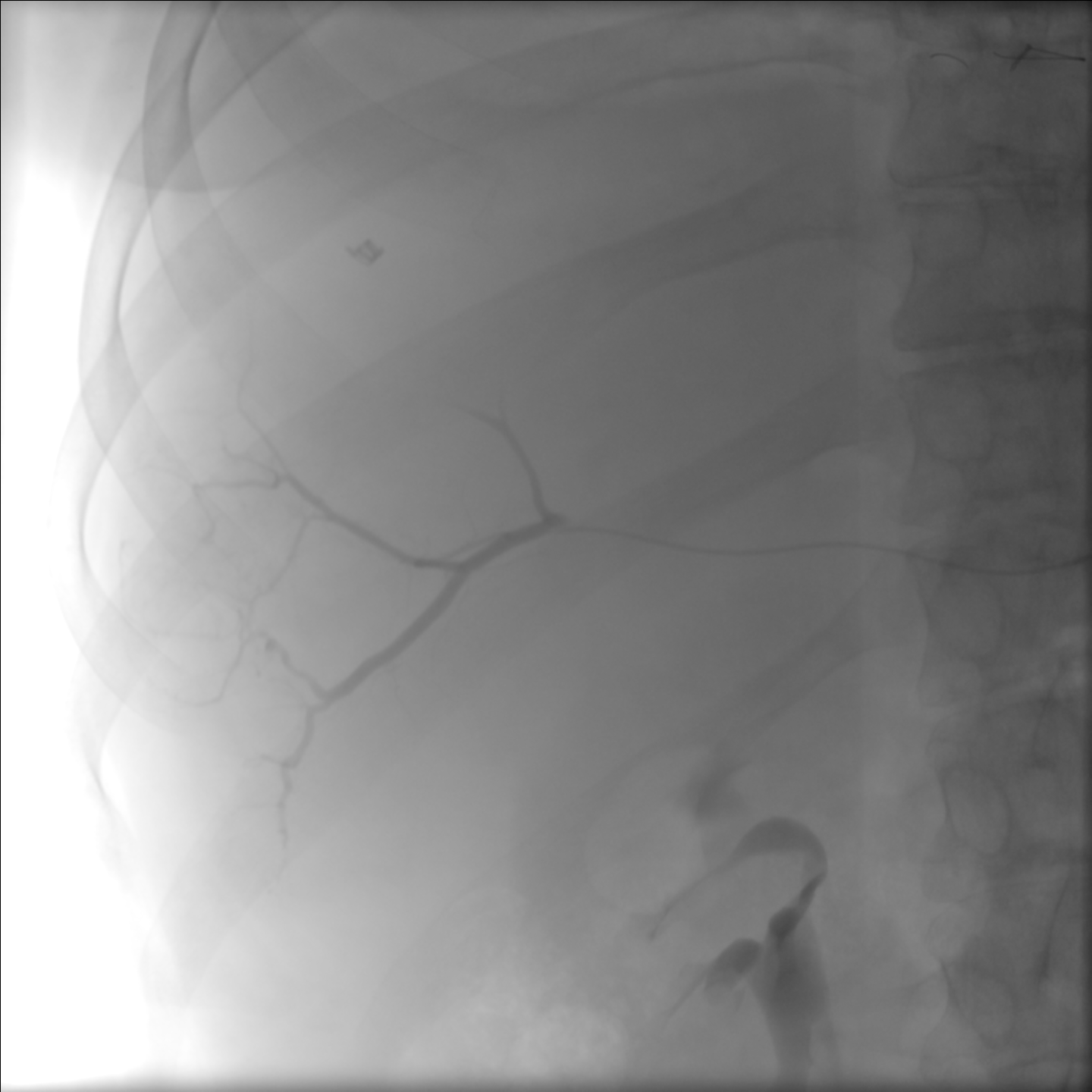
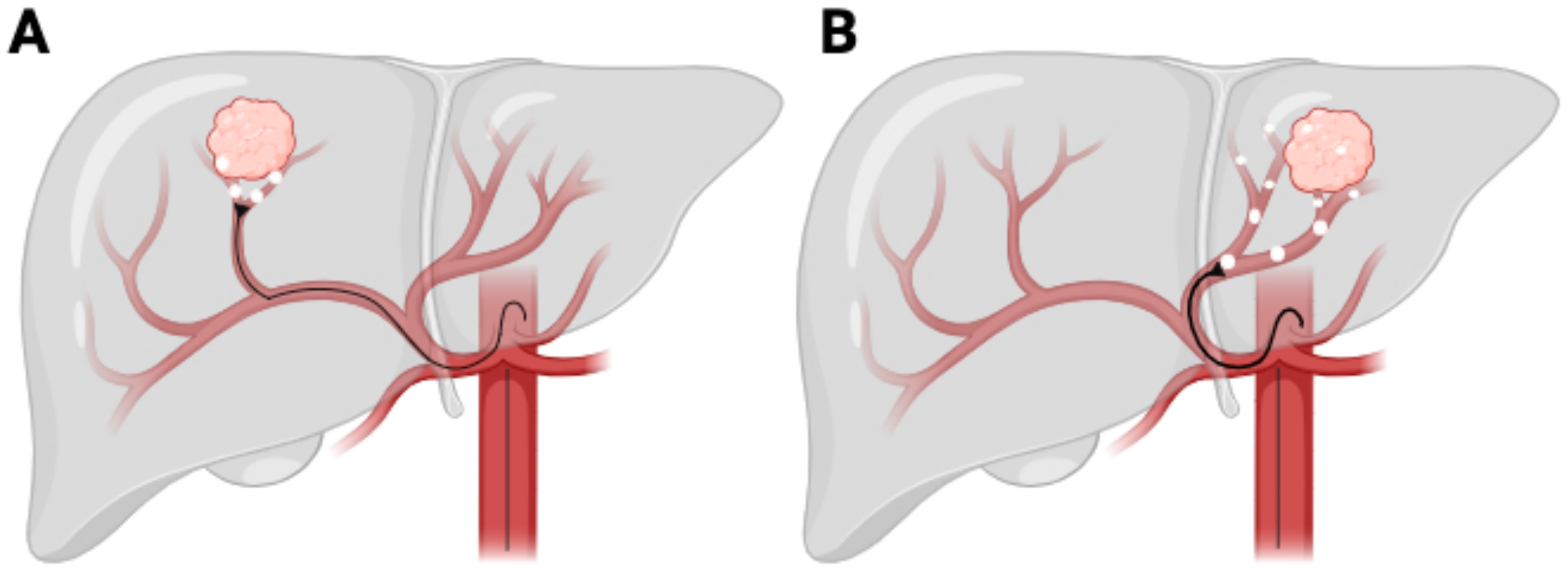
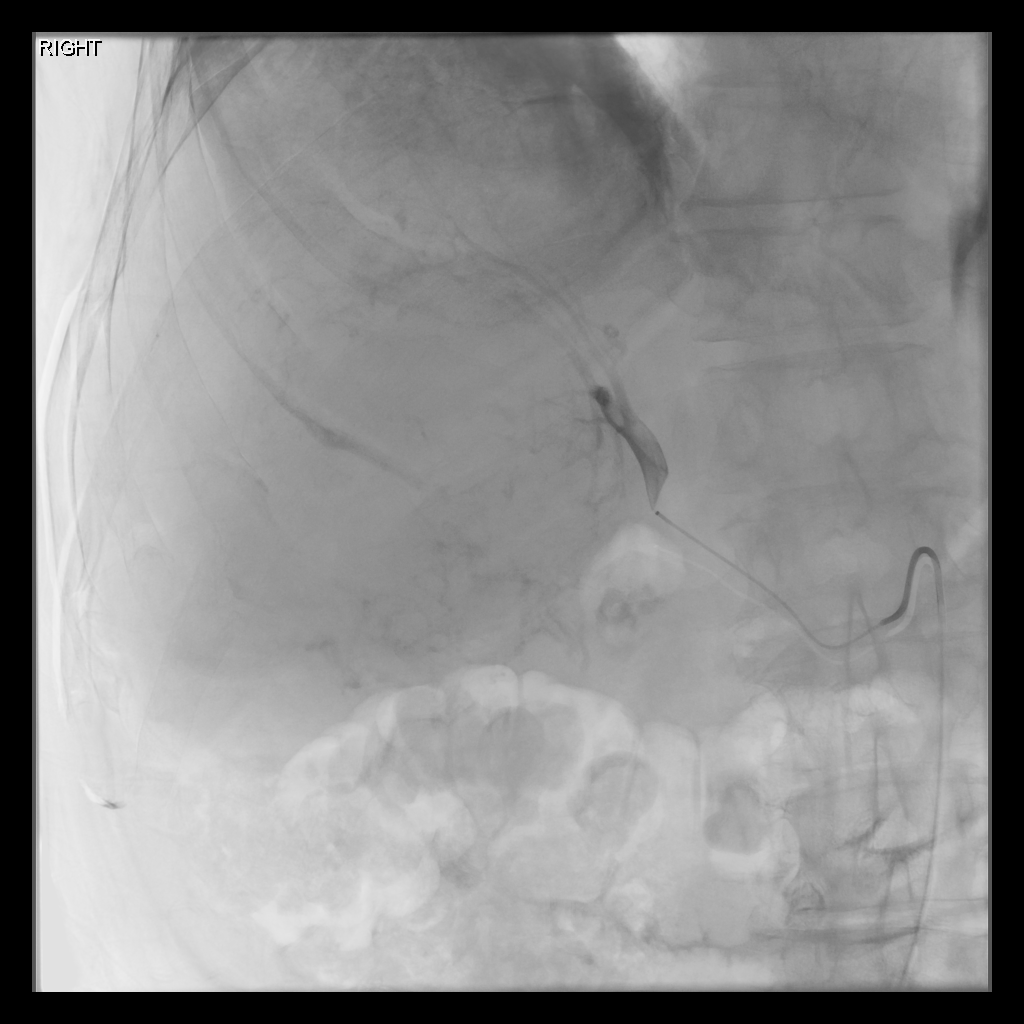
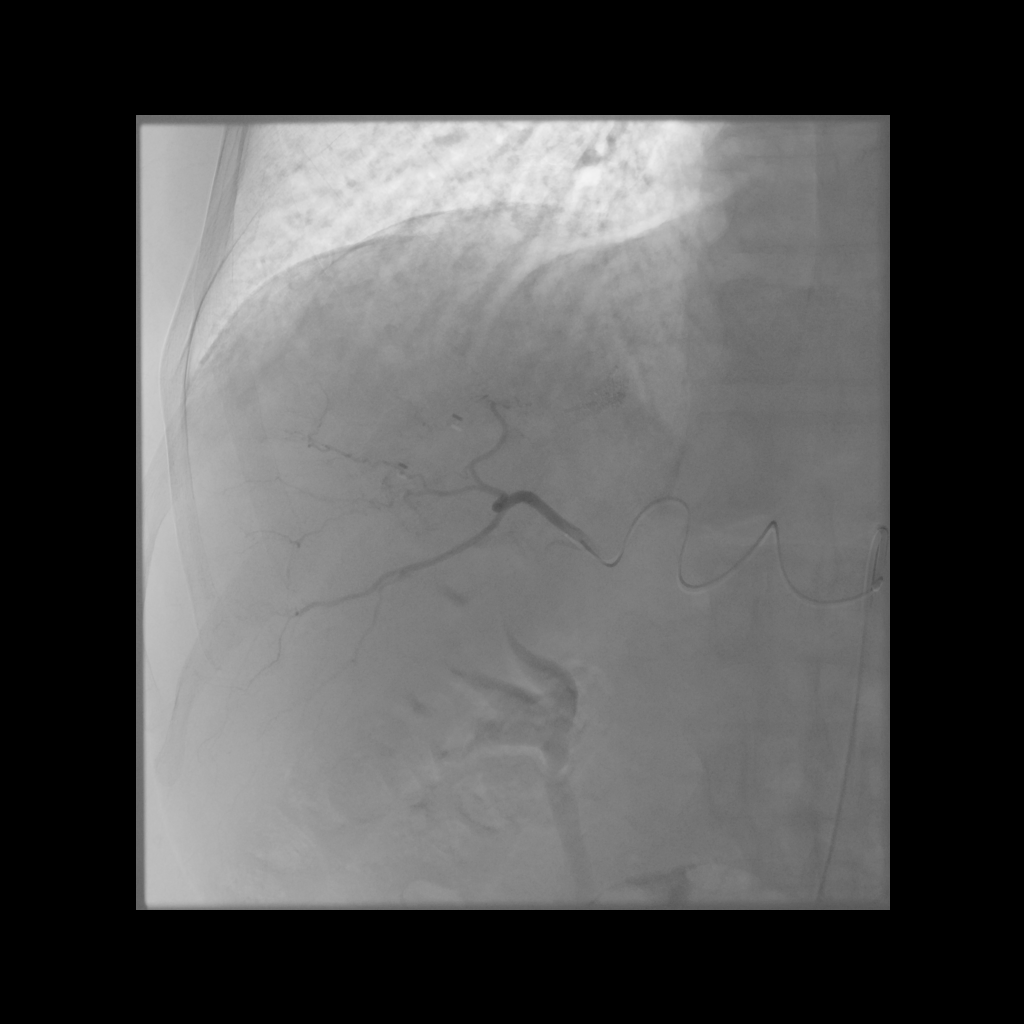
Mapping Angiogram
Comprehensive vascular mapping with CBCT to identify tumor supply and prevent extrahepatic deposition.
Selective catherization
Identify variant hepatic arterial anatomy
Coil embolization of gastroduodenal or right gastric artery
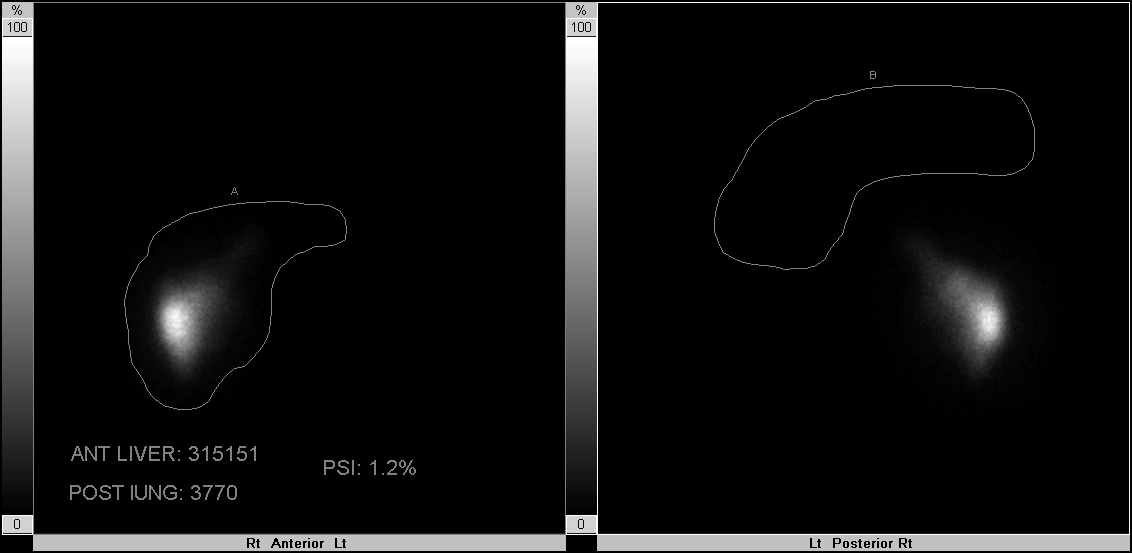
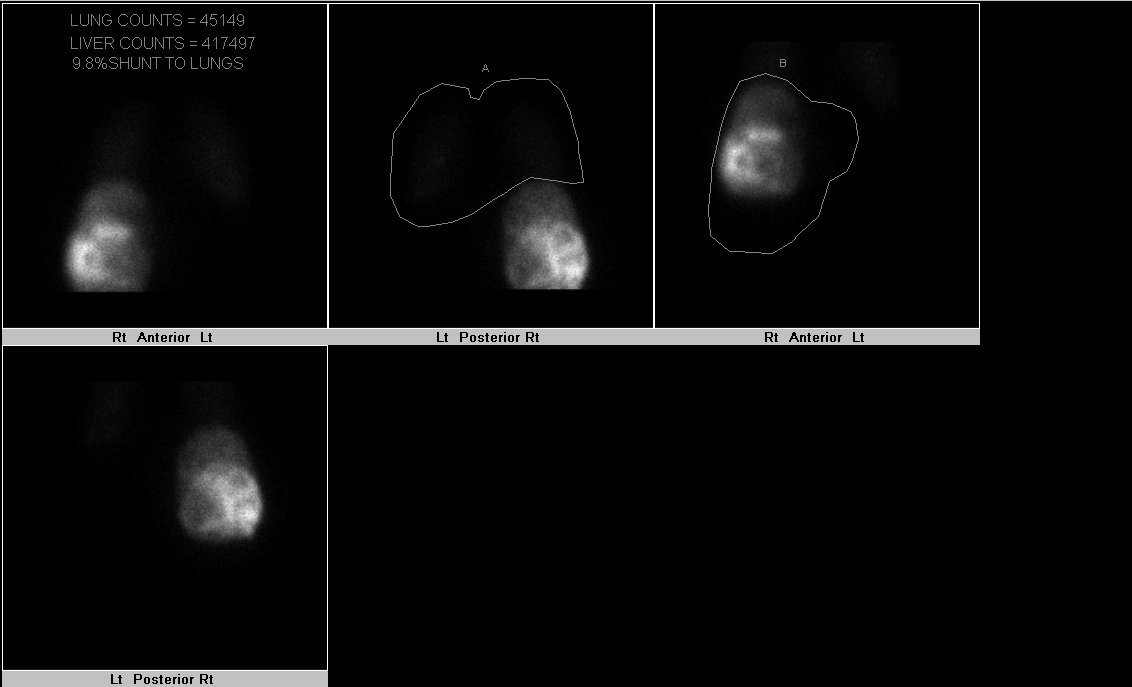
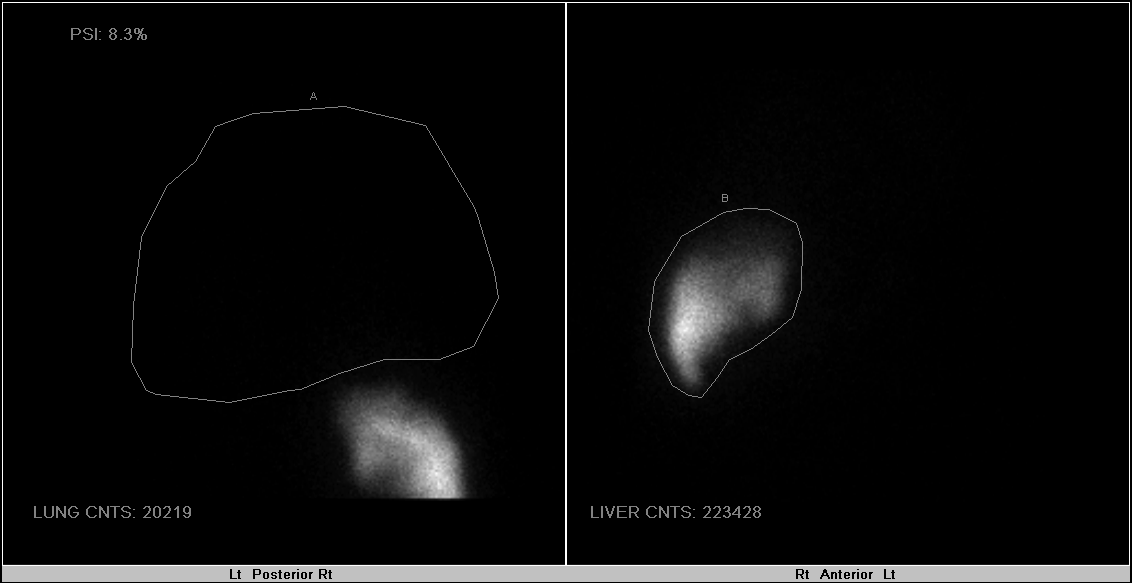
MAA injection to estimate lung shunt and dosimetry
Treatment Day
Selective catheterization
Deliver microspheres slowly under fluoroscopy
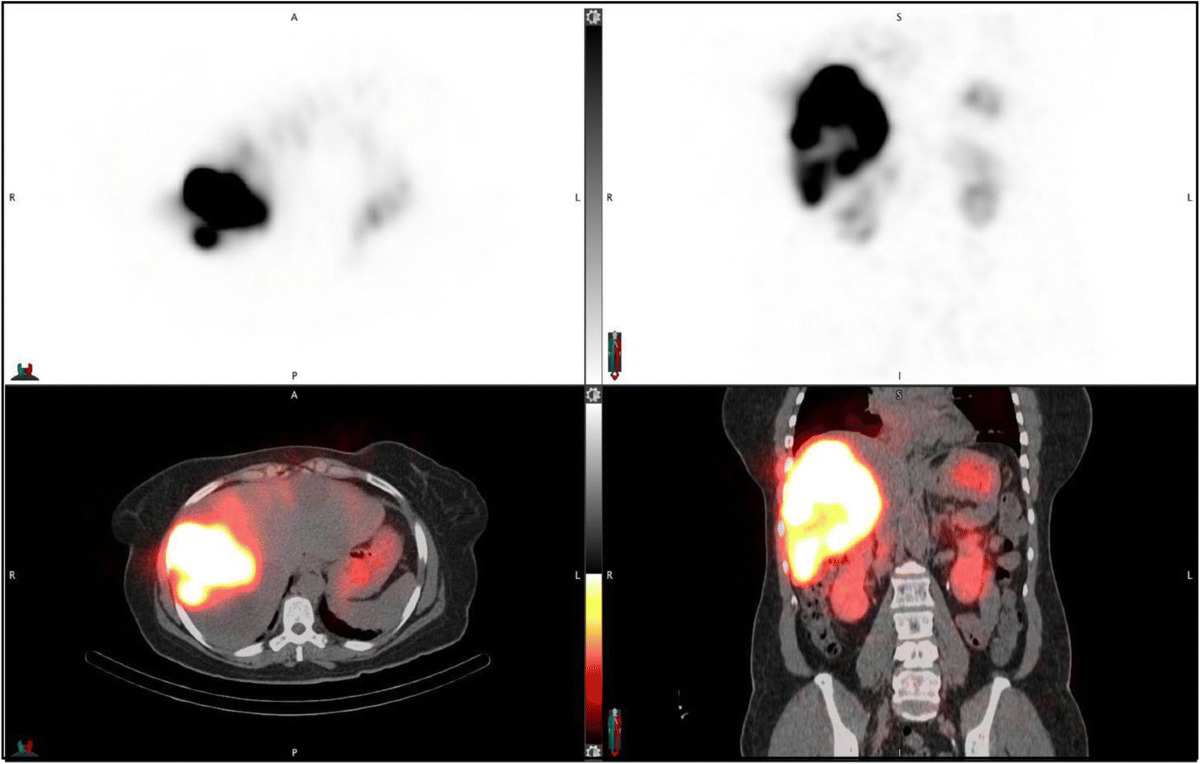
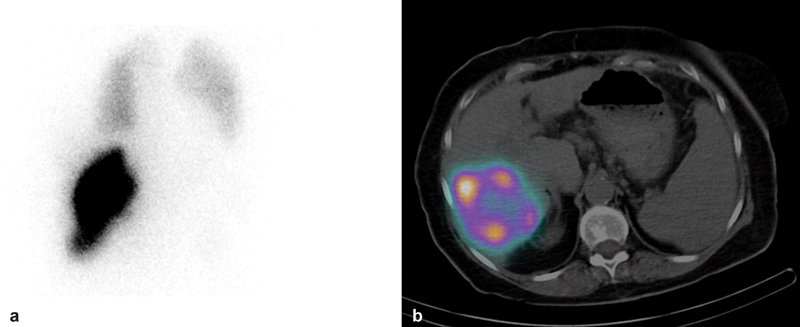
Post-treatment SPECT or PET imaging
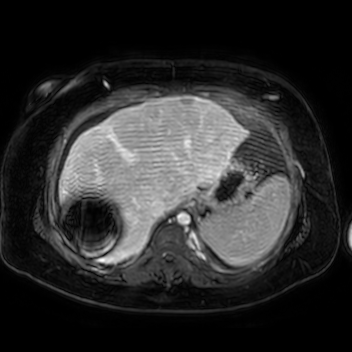
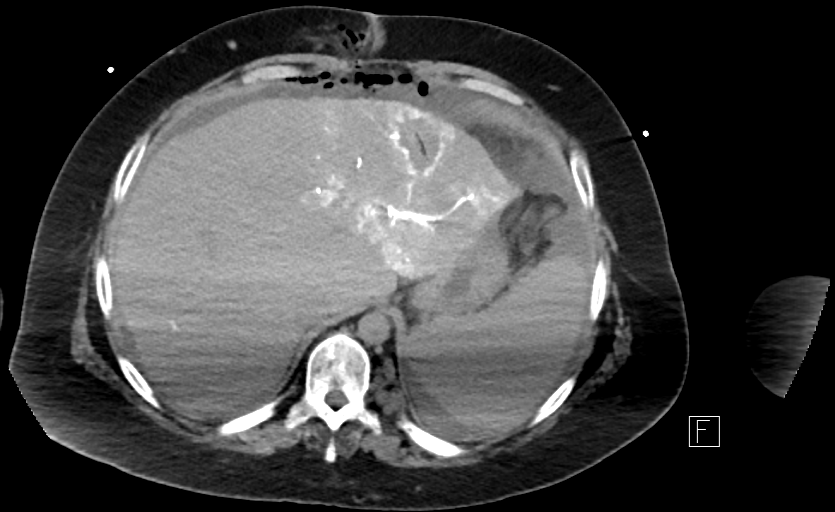
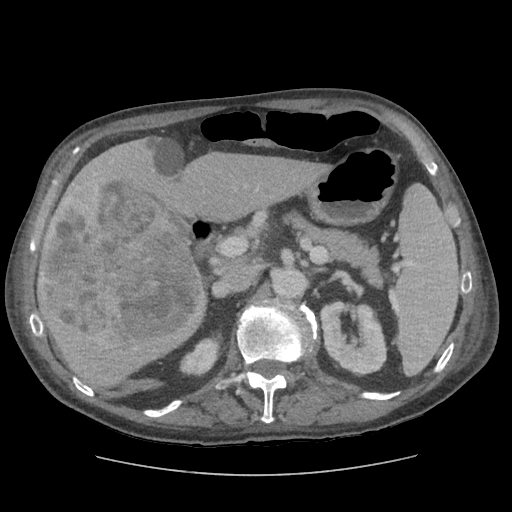
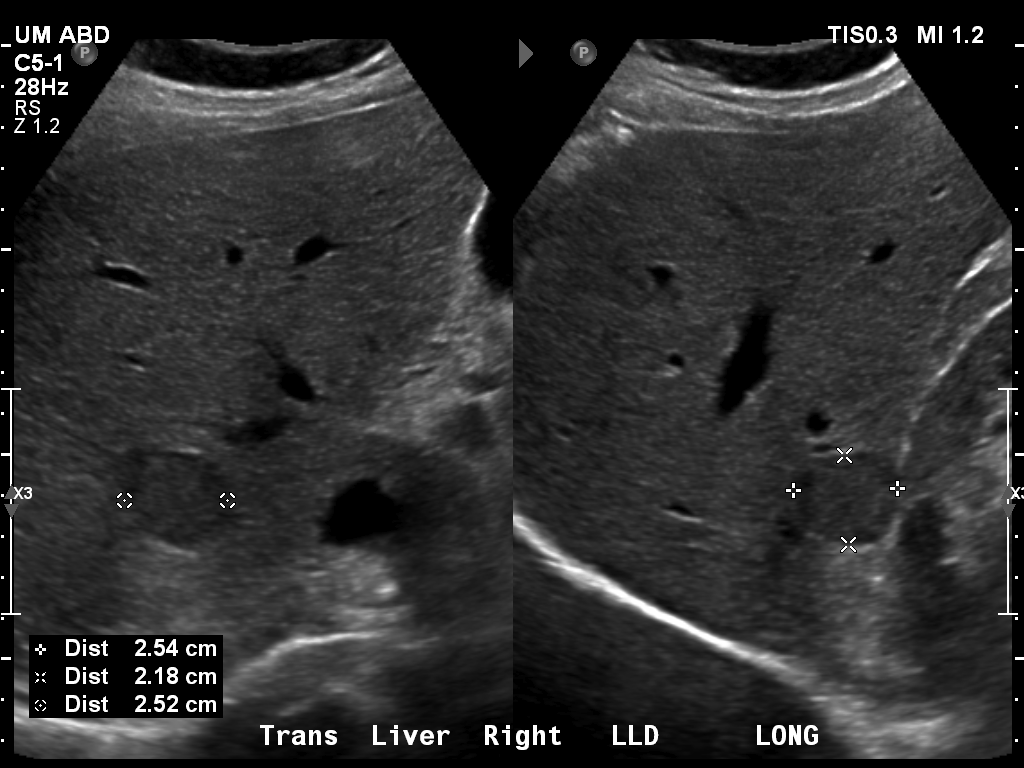
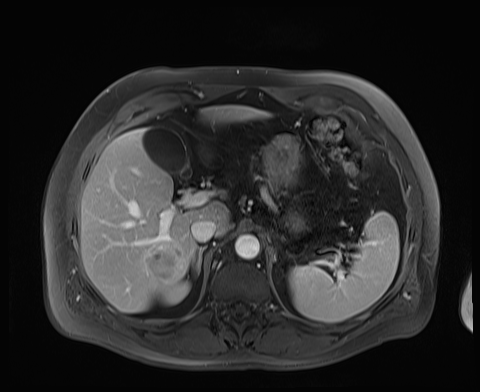
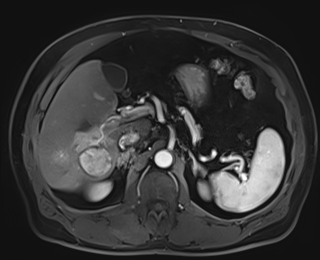
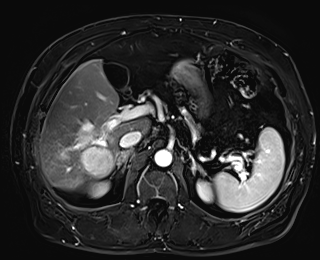
Case 1
79 M with PMH of CKD, HLD, prostate cancer s/p prostatectomy + radiation presenting with feelings of fogginess, upset stomach, and diarrhea. Originally worked up at OSH, imaging concerning for a hepatic mass.
148/77 mmHg / 95 bpm / 15 breaths/min / 98.1°F / 98 ORA
sclera anicteric, no jaundice
AST 112, ALT 34, Alk Phos 202, CEA 2, CA 19-9 4






Case 2


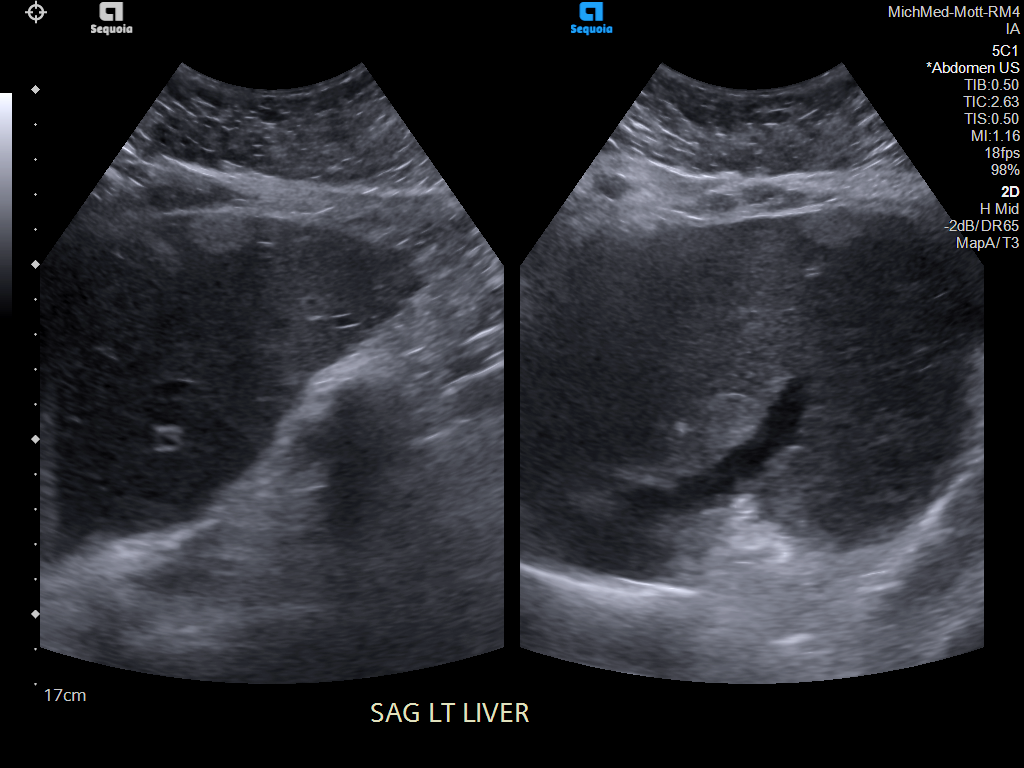
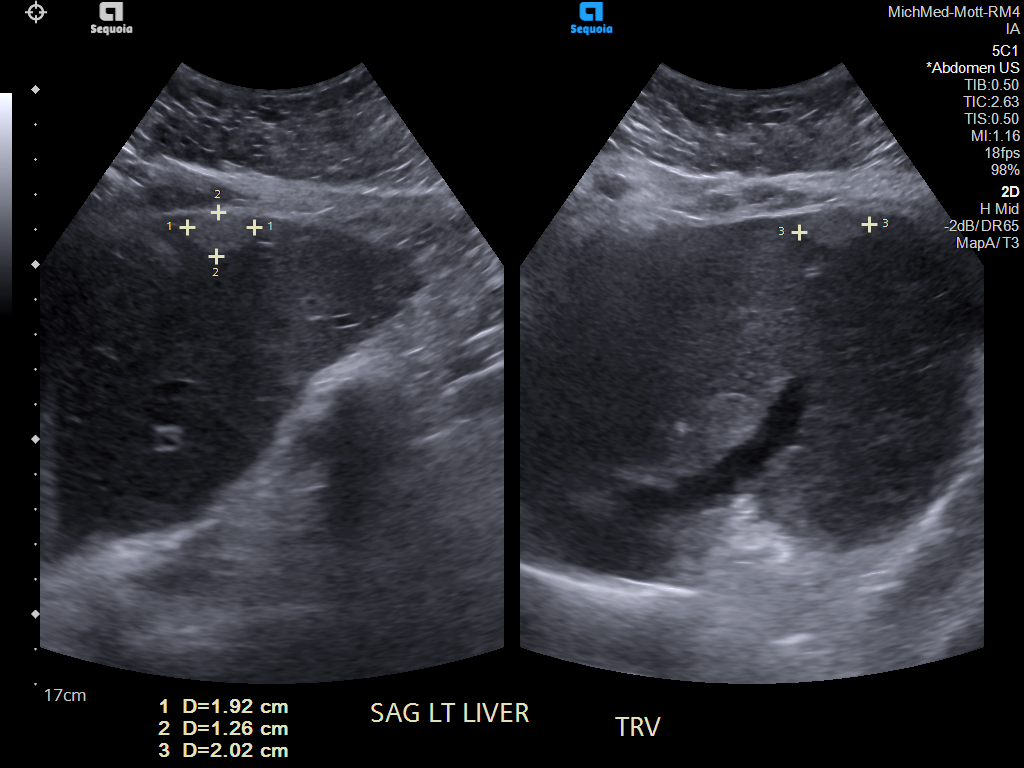
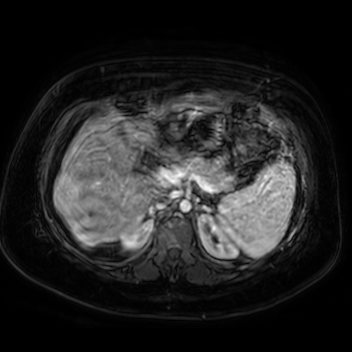
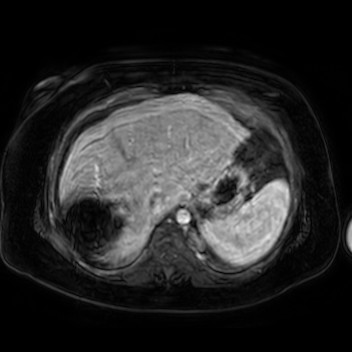
Case 3
20 F with PMH hypoplastic left heart s/p fenestrated Fontan procedure admitted for shortness of breath and hypoxia of uncear etiology.
145/58 mmHg / 78 bpm / 20 breaths/min / 97.6°F / 88% 6L
Faint expiratory wheezing in upper lungs, rhinorrhea, and congestion
AST 33, ALT 33, Alk Phos 222