Fibroid Care
Uterine Artery Embolization
in Modern Gynecology

Indiana University School of Medicine
February 24, 2026
Clinical Challenge
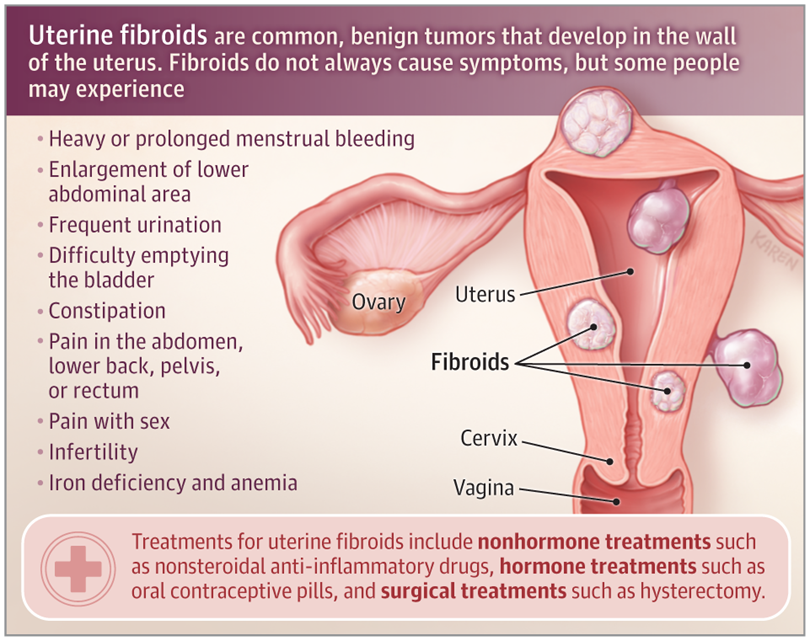
Uterine fibroids are the most common benign neoplasia of reproductive age, creating a substantial burden for millions of women
Affects up to 60-70% of all women by age 50.
Over 80% of African American women are diagnosed by the age of 50.
African American women experience an earlier onset, higher cumulative risk, larger and more numerous fibroids, and more severe symptoms.
African American women are 2-3 times more likely to undergo a hysterectomy and 6.8 times more likely to undergo a myomectomy
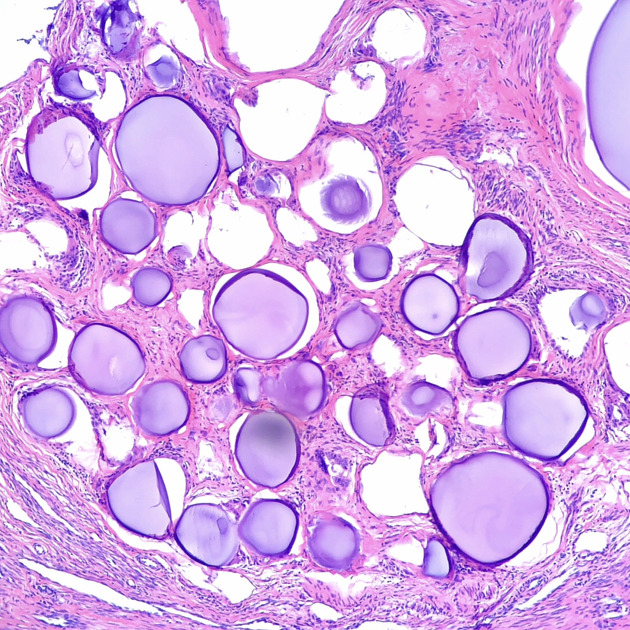
Uterine fibroid types

FIGO Classification System
Other Group
Type 0: pedunculated intracavitary
Type 1: <50% intramural
Type 2: ≥50% intramural
Type 3: 100% intramural; contacts endometrium
Type 4: intramural
Type 5: subserosal ≥50% intramural
Type 6: subserosal <50% intramural
Type 7: subserosal pedunculated
Type 8: other, e.g. cervical, parasitic
Ultrasound


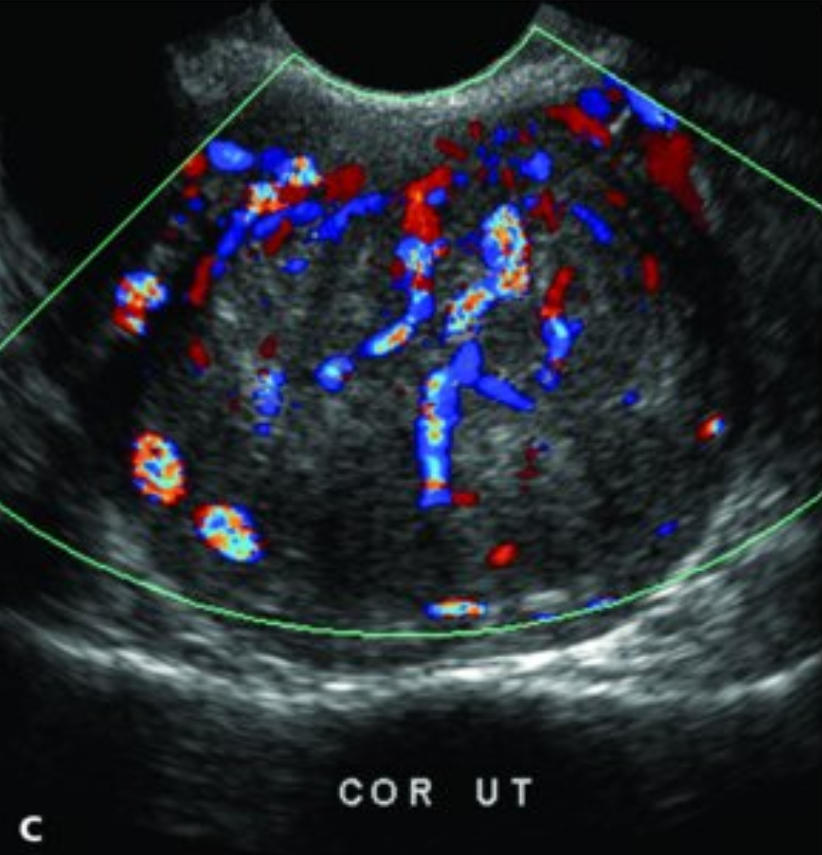
MRI


Pre-Op Requirements
Absolute contraindications:
viable pregnancy
active untreated infection
suspected gynecological malignancy
Relative contraindications:
coagulopathy
severe contrast allergy
severe renal impairement
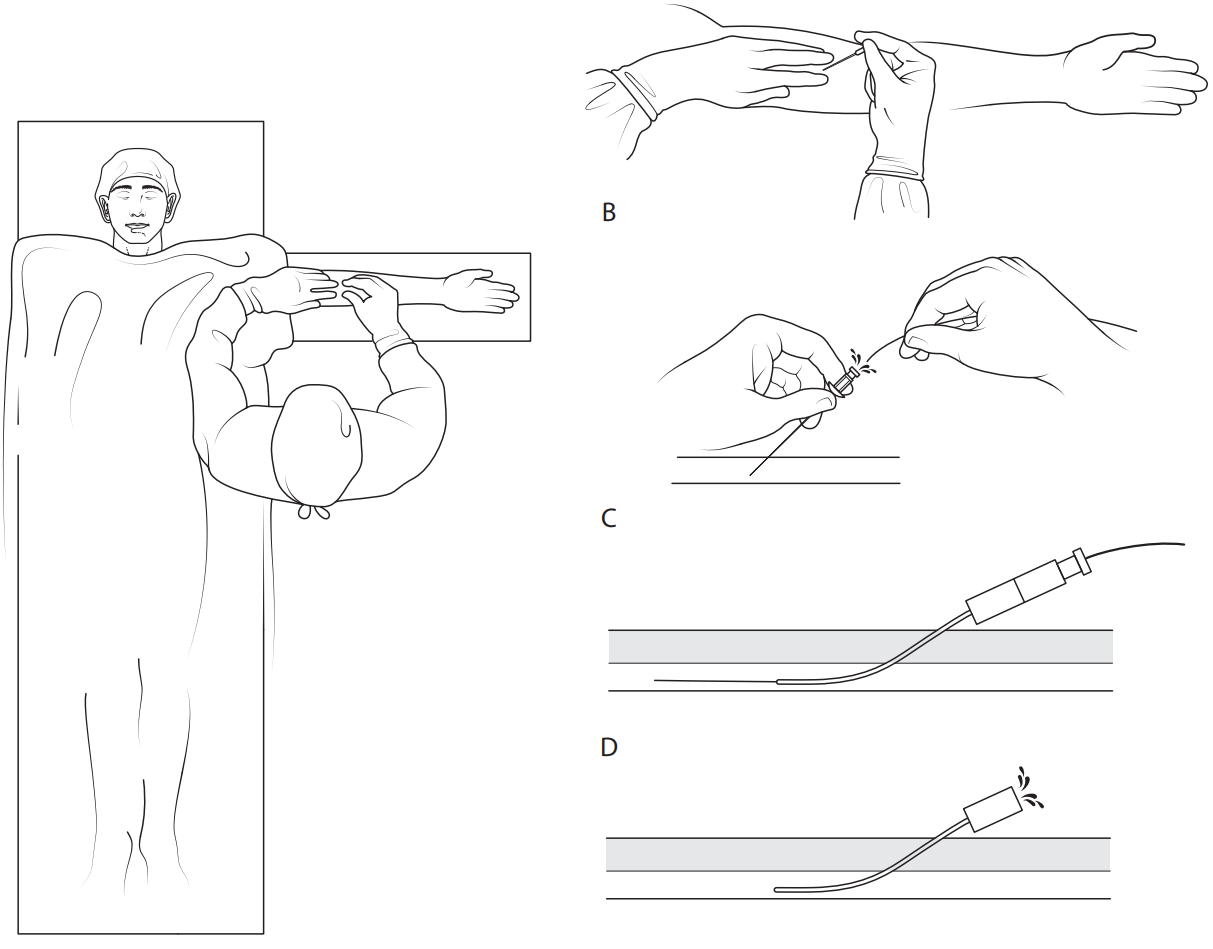
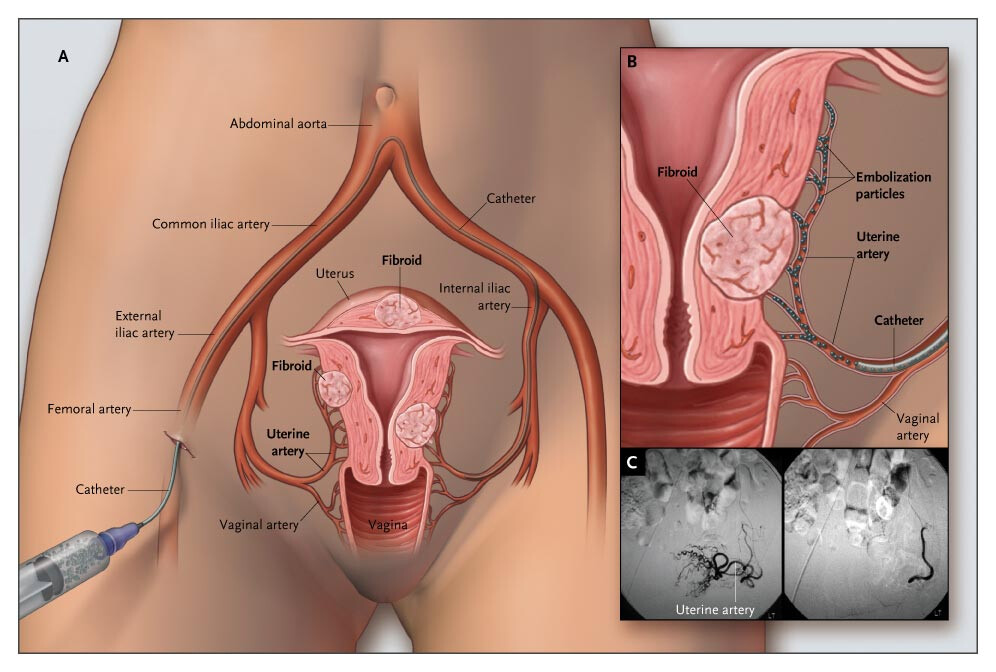
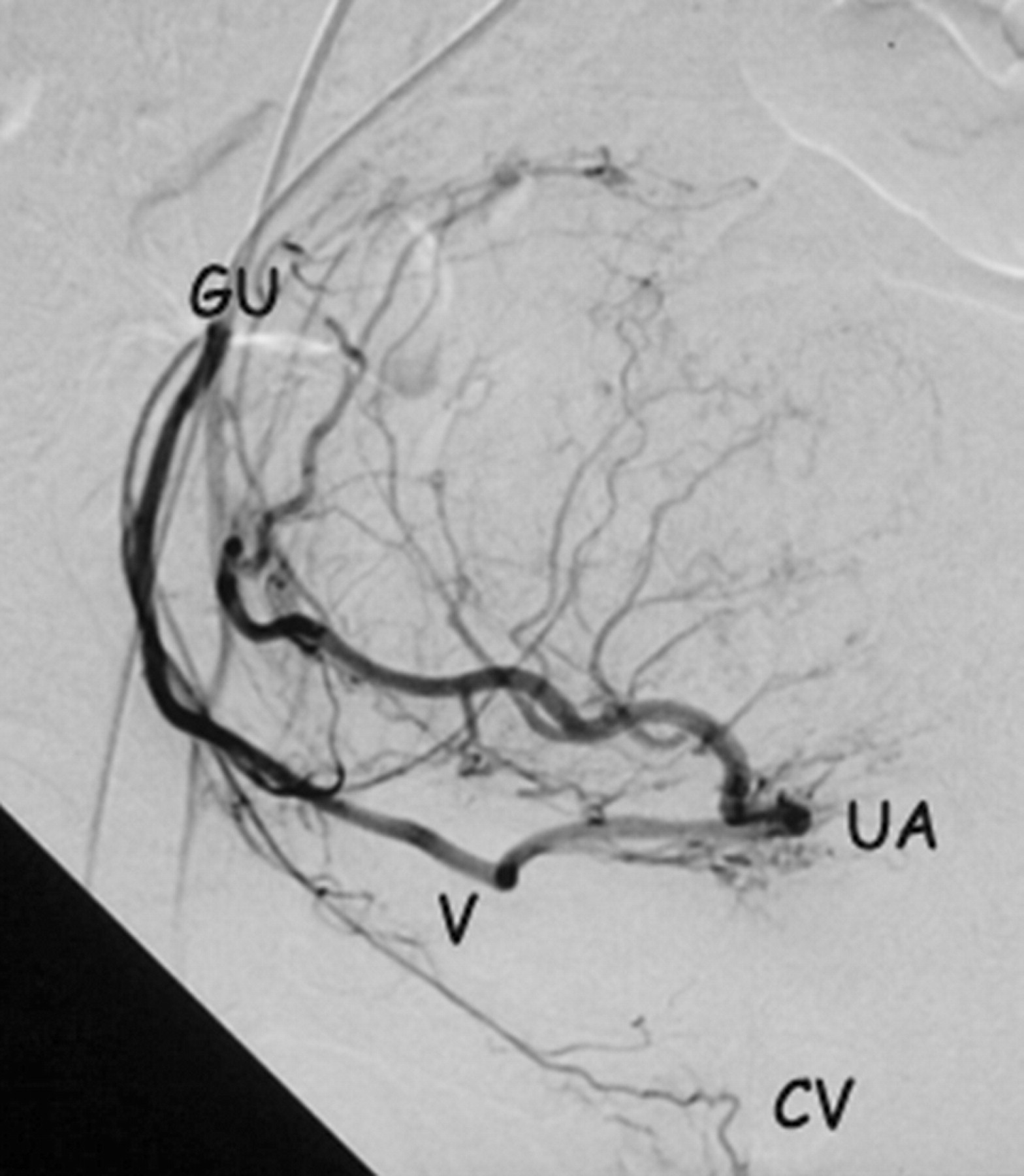
Procedure
Vascular access:
Common femoral artery (traditional)
Radial artery (newer)
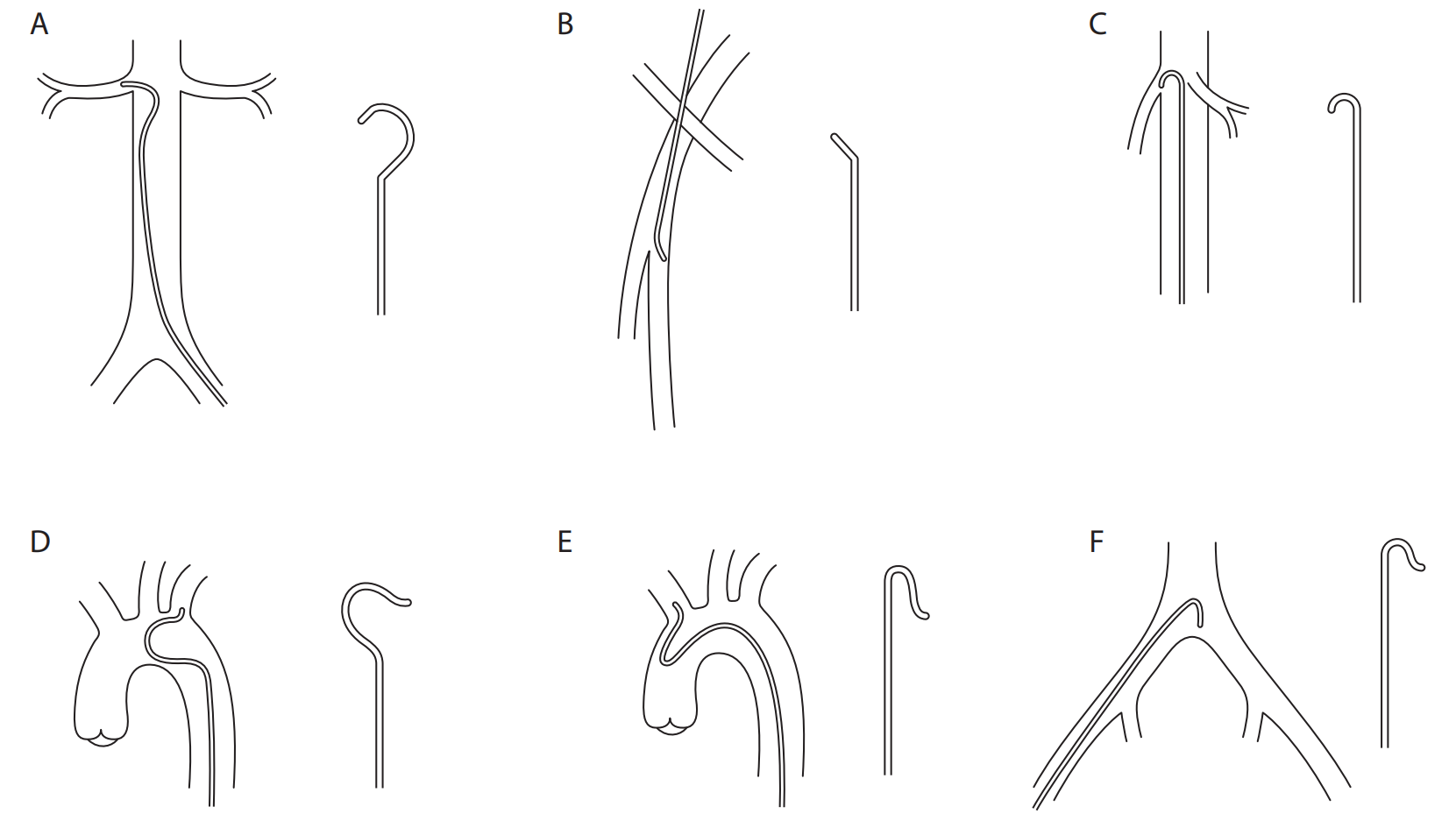
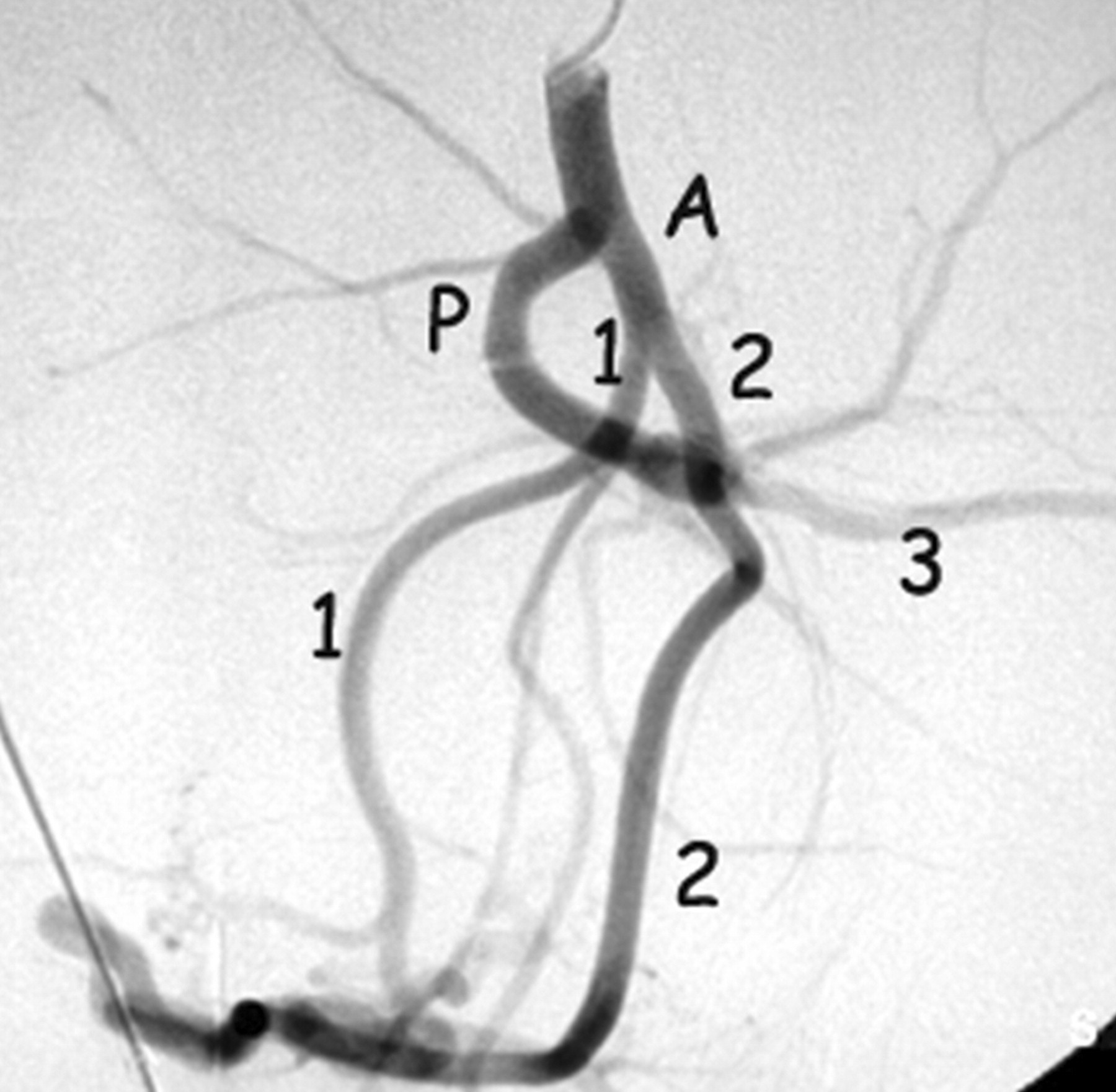
Path
- Aorta -> Common Iliac -> Internal Iliac -> Anterior Division -> Uterine Artery
Procedure
Vascular access:
Common femoral artery (traditional)
Radial artery (newer)
Path
- Aorta -> Common Iliac -> Internal Iliac -> Anterior Division -> Uterine Artery
Procedure
Vascular access:
Common femoral artery (traditional)
Radial artery (newer)
Path
- Aorta -> Common Iliac -> Internal Iliac -> Anterior Division -> Uterine Artery
Complications
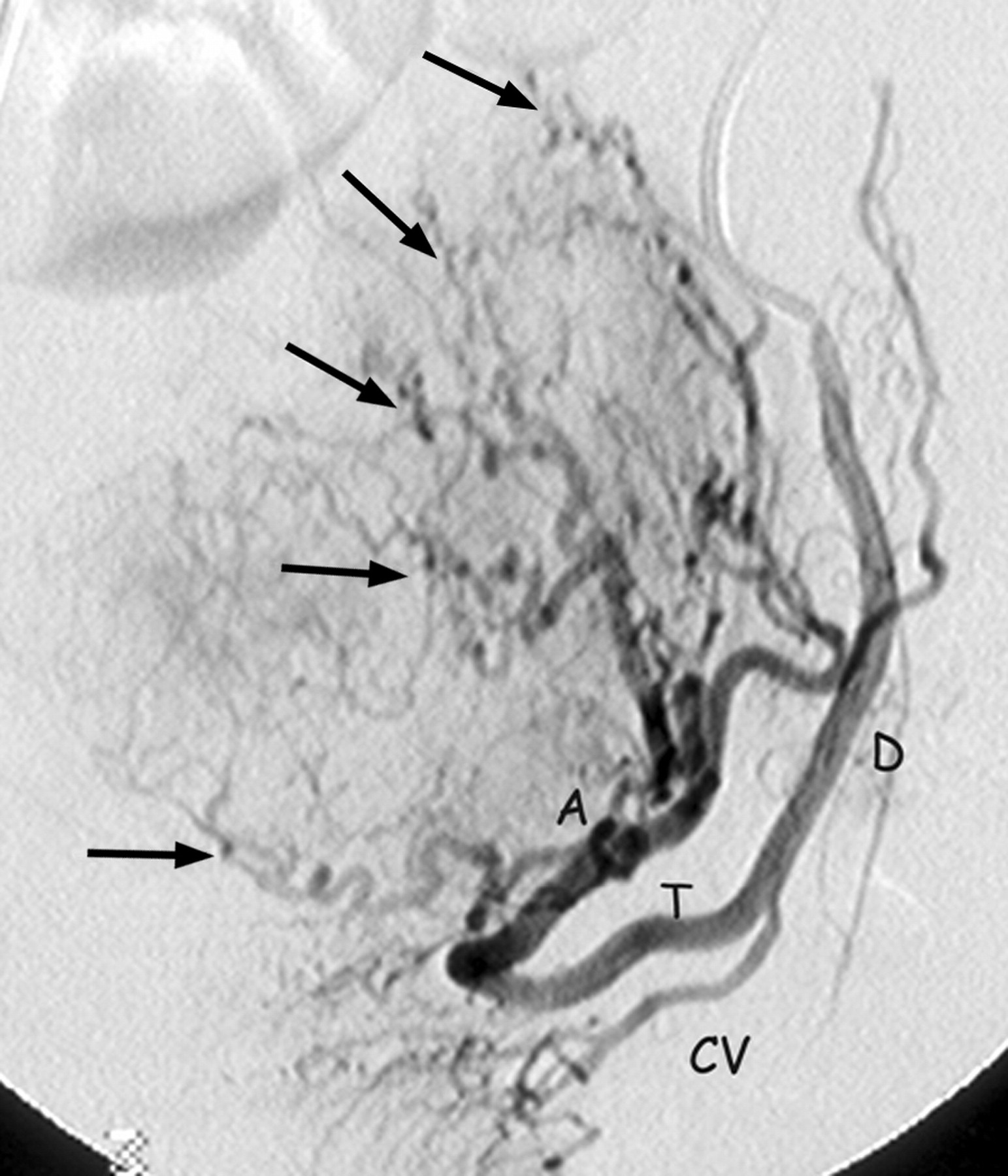
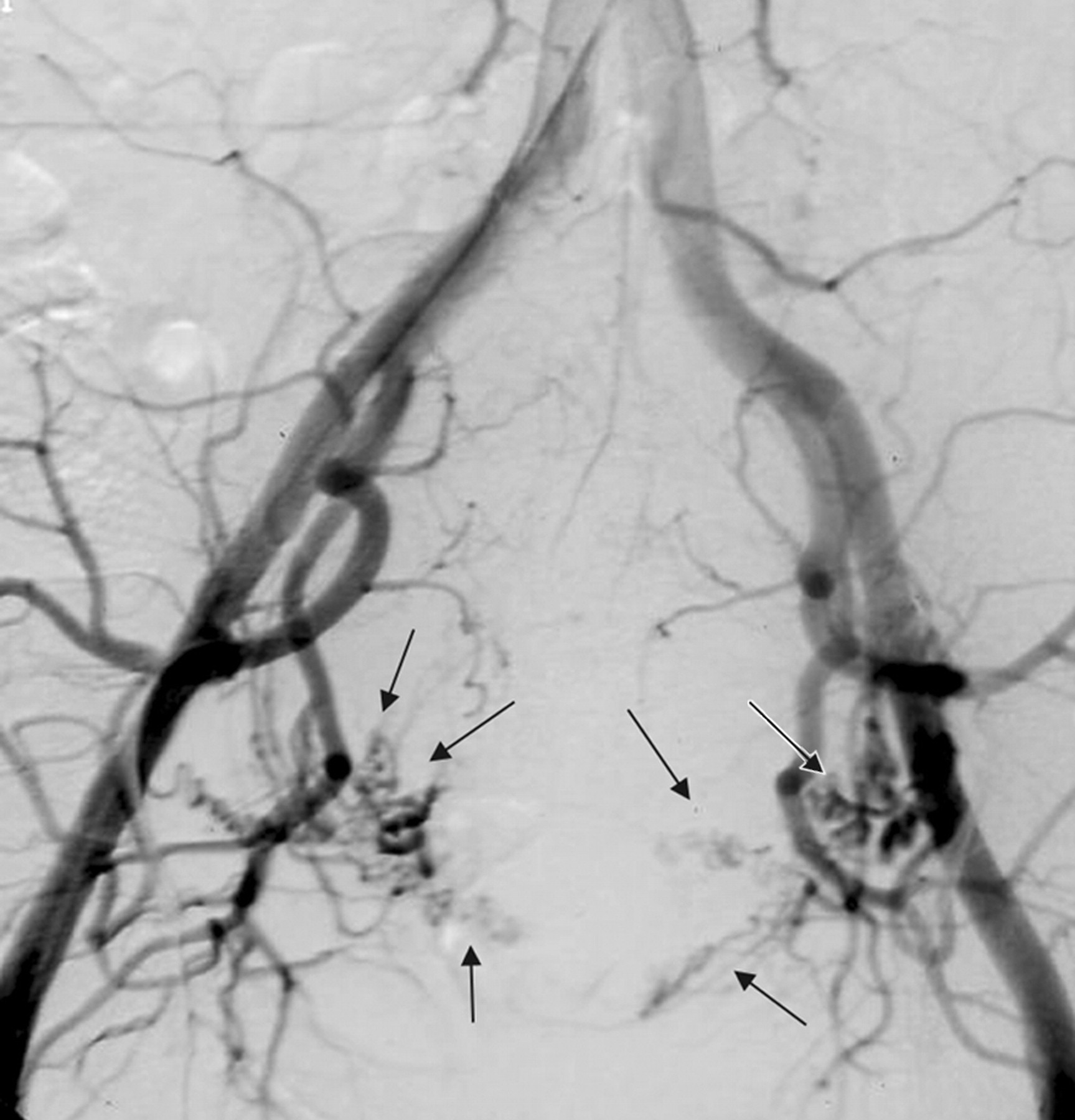
Utero-ovarian anastomosis: 1-5% risk of premature ovarian failure
Gluteal artery: risk of skin necrosis
Vaginal artery: risk of necrosis
Quality of Life and Symptom Control
Multiple meta-analyses of RCTs have compared patient-reported outcomes between UAE and myomectomy.
- Quality of Life: Both procedures lead to substantial improvements in health-related quality of life, with little to no significant difference between the two at 2- and 4-year follow-up.

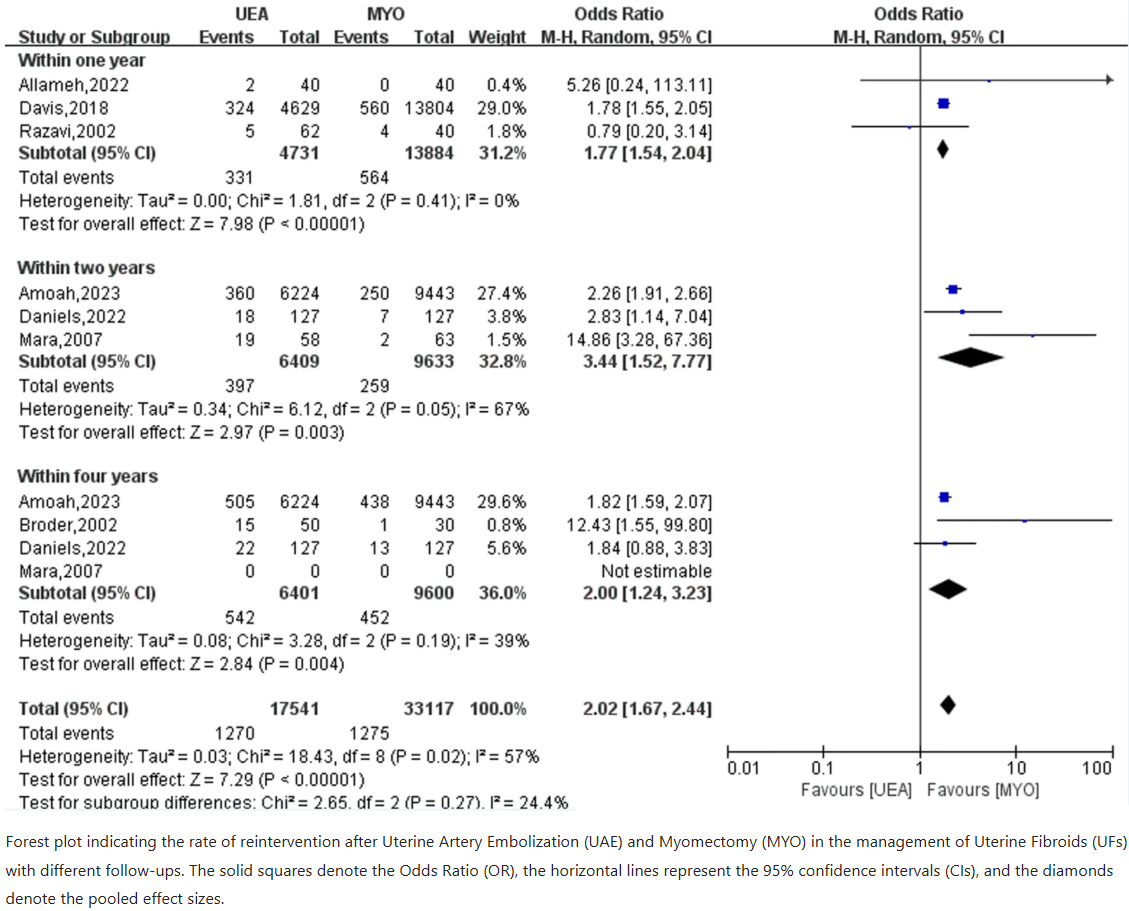
Durability
- Meta-analyses consistently show that myomectomy is associated with significantly lower risk of reintervention compared to UAE. (RR 0.32 favoring myomectomy).

The long-term rate of subsequent hysterectomy is also higher in the UAE group.
Fertility
The effect of UAE on future fertility is one of the most debated aspects of the procedure. While successful pregnancies are well-documented post-UAE, significant uncertanties remain.
Current Consensus
Standard of Care: Myomectomy remains the leading recommended treatment for women with fibroids who wish to conceive (ACOG, CNGOF).
Pregnancy rates: Meta-analyses show either a decreased postoperative pregnancy rate after UAE or no statistically significant difference compared to myomectomy.
Obstetric risk: Several studies report an incresed risk of miscarriage, placental abnormalities (previa, accreta), and postpartum hemorrhage following UAE. A 2008 RCT noted a micarriage rate of 64% in UAE groups, though the trial had limitations.

Treatment Gap Between Patient Preferences and Clinical Reality
Despite a preference for non-surgical and uterine-sparing treatments, particularly among Black women, hysterectomy remains a dominant therapy.
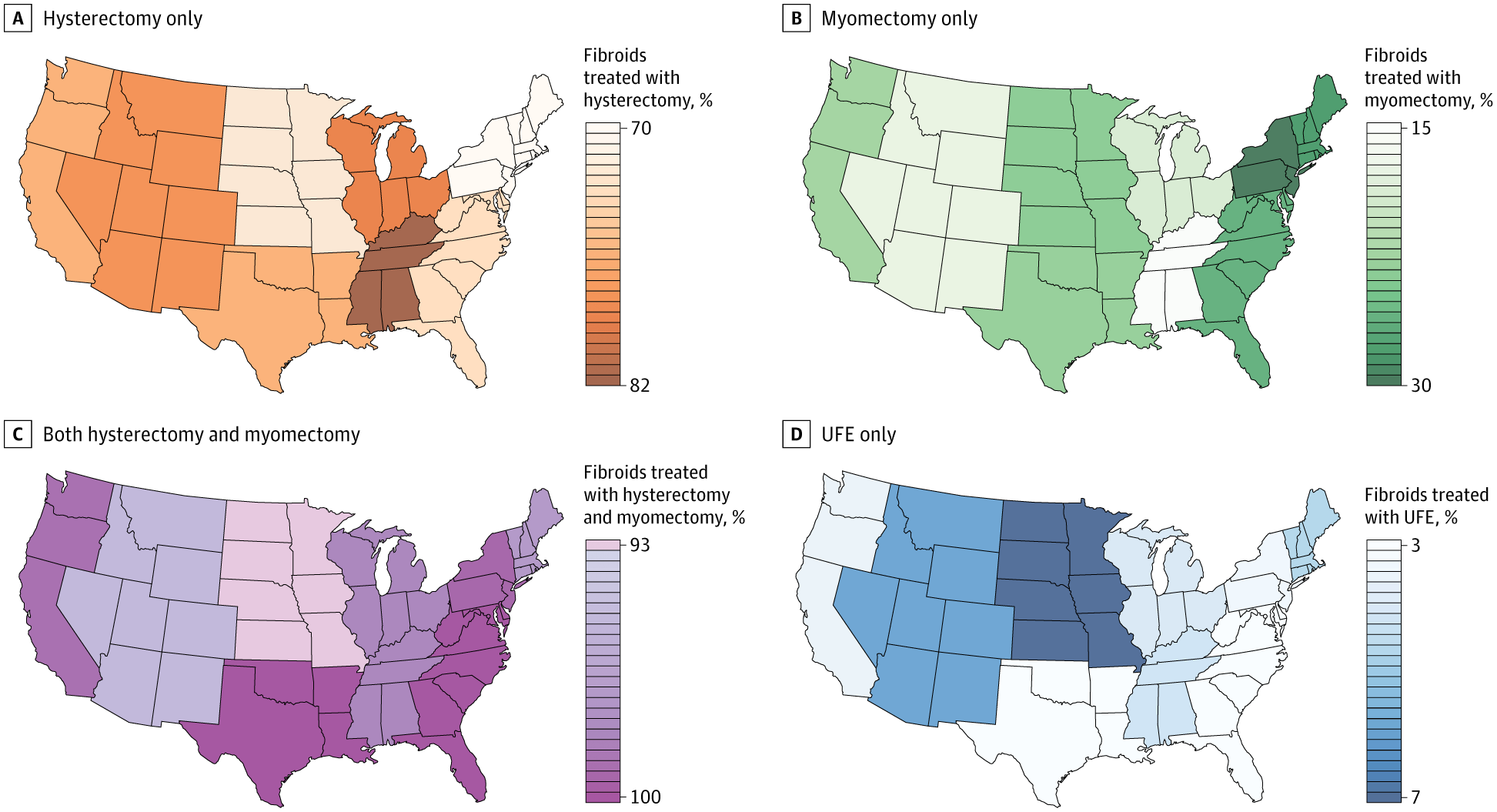
Hysterectomy is the only definitive, but most invasive treatment and results in infertility. Myomectomy preserves the uterus but involves myometrial traua and adhesions.
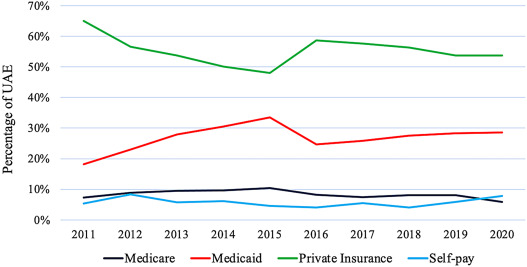
Women with lower socioeconomic status are more likely to receive invasive treatments. This may be due to delaying care until symptoms are severe, limiting less invasive options.
Treatment Gap Between Patient Preferences and Clinical Reality
Despite a preference for non-surgical and uterine-sparing treatments, particularly among Black women, hysterectomy remains a dominant therapy.
Hysterectomy is the only definitive, but most invasive treatment and results in infertility. Myomectomy preserves the uterus but involves myometrial traua and adhesions.
Women with lower socioeconomic status are more likely to receive invasive treatments. This may be due to delaying care until symptoms are severe, limiting less invasive options.

{kind=link}
{kind=link}