Know Before You Go
Anticoagulation and Coagulopathy in Interventional Radiology
Mirindi Kabangu, BS

Indiana University School of Medicine
February 24, 2026
Welcome to the IR Chalk Talk
![]()
Every needle stick, catheter, or wire can cause bleeding.
We need to balance thrombotic risk (why patient is anticoagulated) vs bleeding risk (from procedure)
Pre-Procedure Coagulation Labs: The Basics
Essential labs for most IR procedures (within 30 days unless acute change):
INR: assesses warfarin effect; target <1.5 for high-risk procedures
Platelet count: target >50k for high-risk procedures; >20k may be acceptable for low-risk
aPTT: for heparin monitoring; target <1.5x control for high-risk procedures
Fibrinogen: especially in cirrhosis; target >100 mg/dL for high-risk procedures
Creatinine: for DOAC dosing and clearance; affects hold times
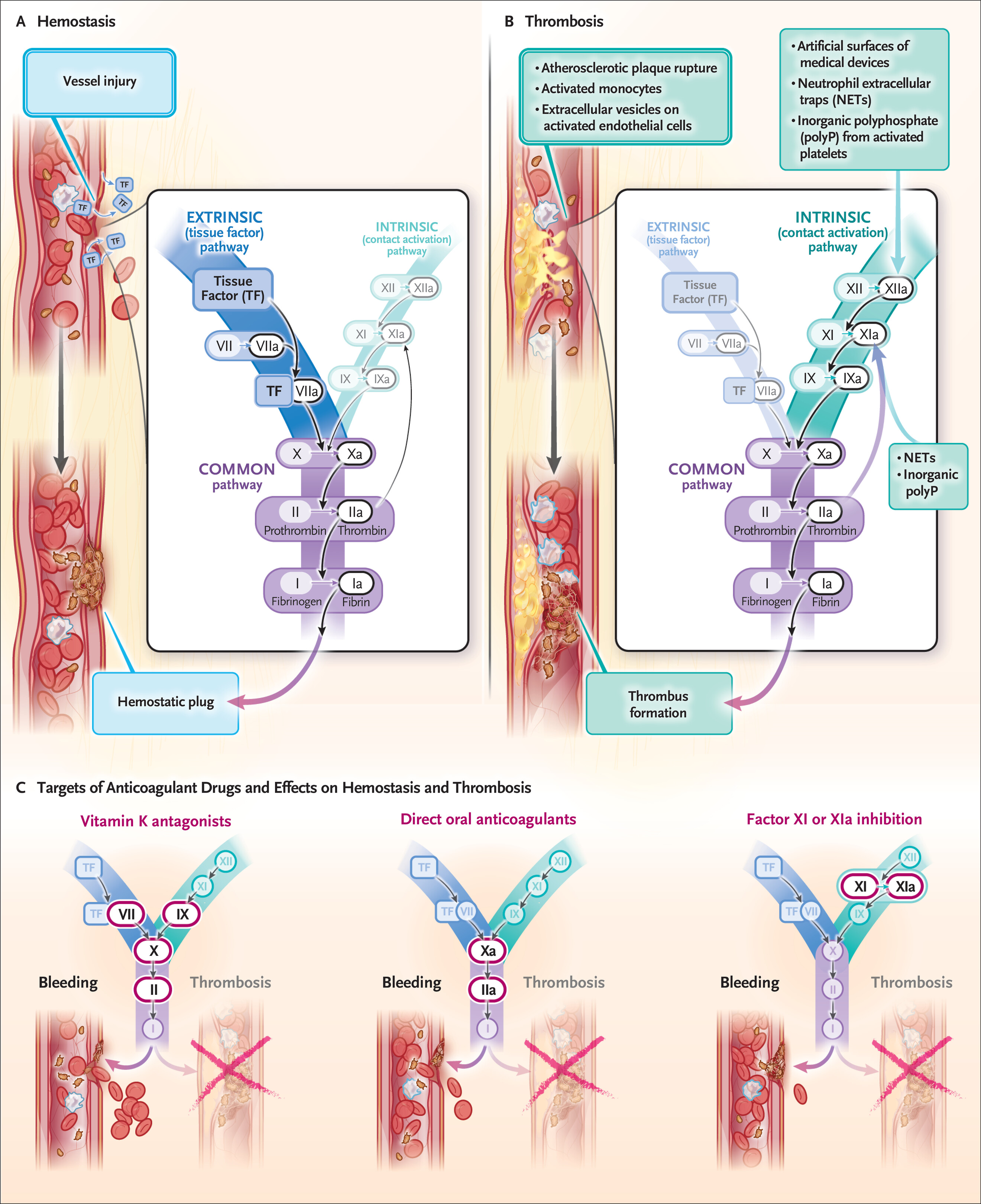
Review
![]()
Common Anticoagulants: Warfarin
coumadin
Mechanism: inhibits vitamin K–dependent factors (II, VII, IX, X, proteins C and S)
Half‑life: 36-40 hours
Reversal: Vitamin K (oral/IV), FFP, PCC (4‑factor)
Common Anticoagulants: DOACs
apixaban, rivaroxaban, edoxaban, dabigatran
Mechanism: Direct factor Xa or IIa inhibitors
Half‑life: 5‑15 hours (renal dependent)
Reversal: Andexanet alfa (Xa), idarucizumab (dabigatran), or PCC 25-50 U/kg off‑label
Note: DOACs have shorter half-lives than warfarin, but renal impairment can prolong clearance
Antiplatelet Agents: Aspirin
aspirin
Mechanism: Irreversible COX inhibitor, inhibits platelet aggregation
Half-life: 7-10 days (platelet lifespan)
Reversal: Platelet transfusion may be considered, but evidence is limited and may not be effective
Antiplatelet Agents: P2Y12 Inhibitors
clopidogrel, prasugrel, ticagrelor
Mechanism: Inhibit ADP-mediated platelet activation
Half-life: clopidogrel/prasugrel 7-10 days, ticagrelor 3-5 days
Reversal: Platelet transfusion may be considered, but evidence is limited and may not be effective
Risk Stratification for IR Procedures
Low Bleeding Risk: e.g., paracentesis, thoracentesis, superficial biopsies
- usually continue aspirin, INR <3.0, platelets >20k
High Bleeding Risk: e.g., liver biopsy, nephrostomy, arterial interventions
- hold aspirin 5-7 days, INR <1.5, platelets >50k
Case 1: Paracentesis in a Cirrhotic Patient
Scenario: 65-year-old with cirrhosis, tense ascites, INR 1.8, platelets 70. On no anticoagulants.
![]()
Case 1: Paracentesis in a Cirrhotic Patient
Scenario: 65-year-old with cirrhosis, tense ascites, INR 1.8, platelets 70. On no acticoagulants.
Plan: Proceed – paracentesis is low risk.
Evidence: SIR guidelines accept INR ≤ 2.5 and platelets ≥ 20k for low‑risk procedures. Recent NIH review confirms safety with mild-moderate coagulopathy.
Take‑home: Don’t delay therapeutic taps for mild coagulopathy. Use ultrasound guidance.
Case 2: Liver Biopsy on Warfarin
Scenario: 62F with hepatitis C, needs liver biopsy. On warfarin for AFib (CHADS2‑VASc 3). INR 2.8.
![]()
Case 2: Liver Biopsy on Warfarin
Scenario: 62F with hepatitis C, needs liver biopsy. On warfarin for AFib (CHADS2‑VASc 3). INR 2.8.
Plan: - Hold warfarin 5 days
Evidence: SIR guidelines recommend holding warfarin for high‑risk procedures. Recent studies show low thrombotic risk with short-term interruption in AFib.
Take‑home: For high‑risk procedures, hold warfarin and confirm INR. Bridging often not needed for AFib.
Case 3: Nephrostomy on Apixaban
Scenario: 70M with obstructing stone, febrile, pyonephrosis. On apixaban for DVT (CrCl 40).
![]()
Case 3: Nephrostomy on Apixaban
Scenario: 70M with obstructing stone, febrile, pyonephrosis. On apixaban for DVT.
Plan: - Emergent nephrostomy needed
Hold apixaban, but proceed with procedure
Reversal options: Andexanet alfa (factor Xa inhibitor) or PCC if bleeding occurs
Evidence: SIR guidelines suggest holding DOACs for high‑risk procedures, but in emergencies, proceed with caution. Reversal agents can be considered if bleeding occurs.
Take‑home: In emergencies, prioritize patient stability. Hold DOACs if possible, but don’t delay critical interventions. Know your reversal options.
Correcting Coagulopathy: Agents
Vitamin K: for warfarin reversal, takes 6-12 hours
FFP: provides clotting factors, requires large volume, risk of transfusion reactions
PCC (4‑factor): concentrates factors II, VII, IX, X; rapid reversal of warfarin; off-label for DOACs
Andexanet alfa: specific reversal for factor Xa inhibitors; costly
Idarucizumab: specific reversal for dabigatran; rapid onset
Platelet transfusion: for antiplatelet agents, but evidence is limited and may not be effective
Cryoprecipitate: for fibrinogen replacement in cirrhosis, but evidence is limited
Tranexamic acid: antifibrinolytic, may be considered in bleeding, but evidence in IR is limited
Special Situations
Liver Cirrhosis: coagulopathy is complex; INR may not reflect bleeding risk; consider TEG/ROTEM if available; correction with FFP or cryoprecipitate may be considered for high-risk procedures
Renal Impairment: affects clearance of DOACs; may require longer hold times; consider hemodialysis for dabigatran if urgent reversal needed
Mechanical Heart Valves: high thrombotic risk; usually require bridging with heparin when holding warfarin; consult cardiology
Pediatric Patients: limited data; generally follow adult guidelines but consider age-specific factors and consult pediatric hematology + IR
When to Bridge? (and When Not To)
Bridging: using short-acting anticoagulants (e.g., LMWH) during warfarin interruption to reduce thrombotic risk
Indications for bridging:
When not to bridge:
- BRIDGE trial 1 showed increased bleeding without significant reduction in thrombotic events for AFib patients with moderate stroke risk (CHADS2‑VASc ≤4)